

Dose range evaluation of liposomal nystatin and comparisons with amphotericin B and amphotericin B lipid complex in temporarily neutropenic mice infected with an isolate of Aspergillus fumigatus with reduced susceptibility to amphotericin B
- PMID: 10543734
- PMCID: PMC89530
- DOI: 10.1128/AAC.43.11.2592
Dose range evaluation of liposomal nystatin and comparisons with amphotericin B and amphotericin B lipid complex in temporarily neutropenic mice infected with an isolate of Aspergillus fumigatus with reduced susceptibility to amphotericin B
Abstract
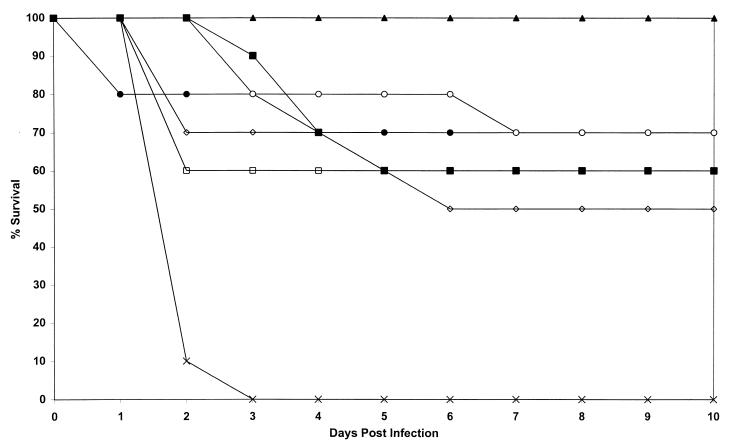
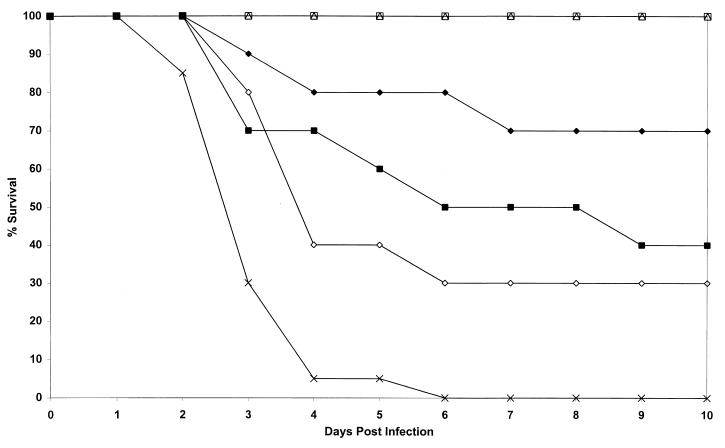
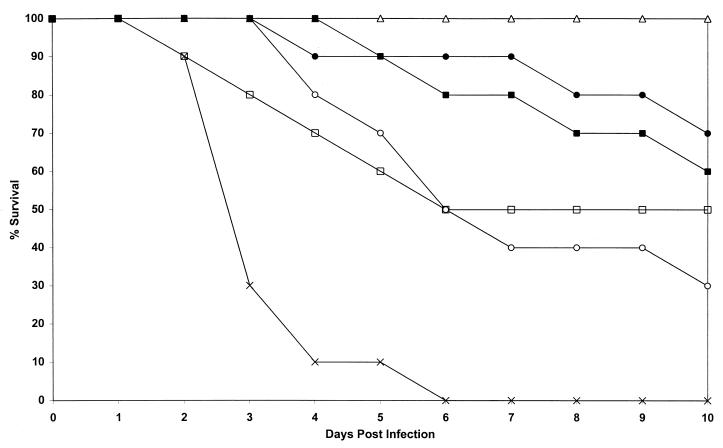
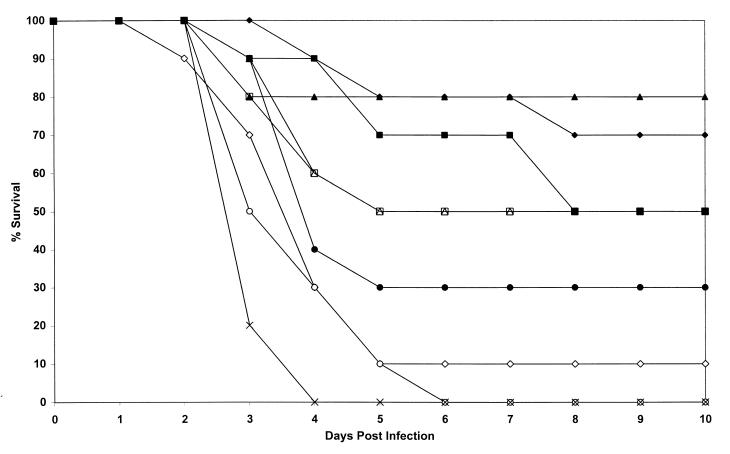
Using an isolate of Aspergillus fumigatus that is less susceptible in vivo to amphotericin B than most other isolates, we compared different doses of liposomal nystatin (L-nystatin), liposomal amphotericin B (L-amphotericin), and amphotericin B lipid complex (ABLC) with amphotericin B deoxycholate. Four experiments with intravenously infected neutropenic mice were conducted. A dose of L-nystatin at 10 mg/kg of body weight was toxic (the mice had fits or respiratory arrest). The optimal dosage of L-nystatin was 5 mg/kg daily on days 1, 2, 4, and 7 (90% survival). This was superior to L-amphotericin (5 mg/kg [P = 0.24] and 1 mg/kg [P < 0.0001]), ABLC (5 mg/kg [P = 0.014] and 1 mg/kg [P < 0.0001]), and amphotericin B deoxycholate (5 mg/kg [P = 0.008]). In terms of liver and kidney cultures, L-nystatin (5 mg/kg) was superior to all other regimens (P = 0.0032 and <0.0001, respectively). Higher doses of L-amphotericin (25 and 50 mg/kg) in one earlier experiment were more effective (100% survival) than 1 mg of L-amphotericin per kg and amphotericin deoxycholate (5 mg/kg) in terms of mortality and both liver and kidney culture results and to L-amphotericin (5 mg/kg) in terms of liver and kidney culture results only. ABLC (25 mg/kg) given daily for 7 days was superior to ABLC (50 mg/kg [P = 0.03]) but not to ABLC at 5 mg/kg or amphotericin B deoxycholate in terms of mortality, although it was in terms of liver and kidney culture results. No dose-response for amphotericin B (5 and 1 mg/kg) was demonstrable. In conclusion, in this stringent model, high doses of L-amphotericin and ABLC could overcome reduced susceptibility to amphotericin B deoxycholate, but all were inferior to 5- to 10-fold lower doses of L-nystatin.
Figures
References
-
- Bowden R, Chandrasekar P, White M, van Burik J A, Wingard J, et al. Abstracts of the International Immunocompromised Host Society Meeting. 1998. A double-blind randomised controlled trial of Amphocil (ABCD) versus amphotericin B (AmB) for treatment of invasive aspergillosis in immunocompromised patients, abstr. 091.
-
- Bowden R A, Cays M, Gooley T, Mamelok R D, van Burik J-A. Phase I study of amphotericin B colloidal dispersion for the treatment of invasive fungal infections after marrow transplant. J Infect Dis. 1996;173:1208–1215. - PubMed
-
- Broughton M C, Bard M, Lees N D. Polyene resistance in ergosterol producing strains of Candida albicans. Mycoses. 1991;34:75–83. - PubMed
-
- Burch P A, Karp J E, Merz W G, Kuhlman J E, Fishman E K. Favourable outcome of invasive aspergillosis in patients with acute leukemia. J Clin Oncol. 1987;5:1985–1993. - PubMed
-
- Caillot D, Casasnovas O, Bernard A, Couailler J F, Durand D, Cuisenier B, Solary E, Piard F, Petrella T, Bonnin A, Couillault G, Dumas M, Guy H. Improved management of invasive pulmonary aspergillosis in neutropenic patients using early thoracic computed tomographic scan and surgery. J Clin Oncol. 1997;15:139–147. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
