

Improved surgical results for hilar cholangiocarcinoma with procedures including major hepatic resection
- PMID: 10561090
- PMCID: PMC1420920
- DOI: 10.1097/00000658-199911000-00008
Improved surgical results for hilar cholangiocarcinoma with procedures including major hepatic resection
Abstract
Objective: To evaluate the long-term outcome of aggressive surgery incorporating hepatic resection and systematic nodal dissection for advanced carcinoma involving the hepatic hilus.
Summary background data: Few long-term results are available regarding radical surgery incorporating major hepatectomy and nodal dissection.
Methods: A retrospective analysis was undertaken in 107 patients with carcinoma involving the hepatic hilus treated between 1980 and 1997. Resectional surgery was performed in 65 patients, 52 of whom underwent major hepatectomies. The effects of clinical and pathologic factors were assessed by univariate and multivariate analyses.
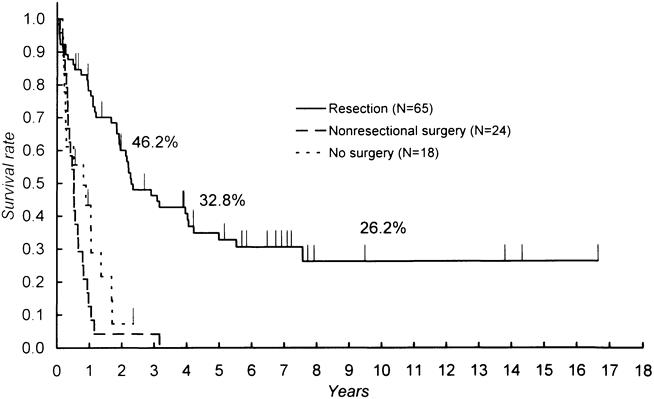
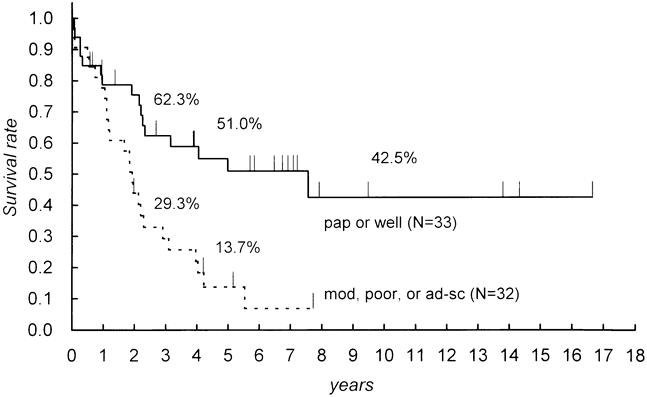
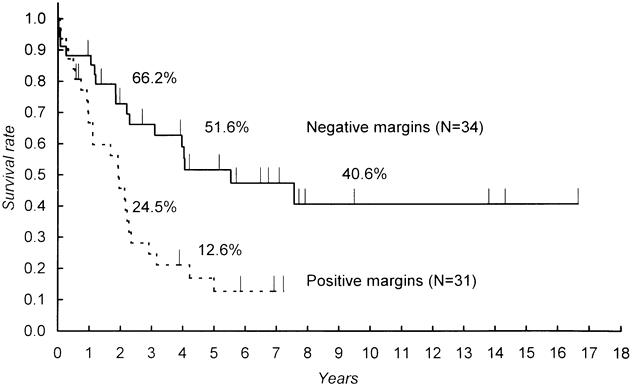
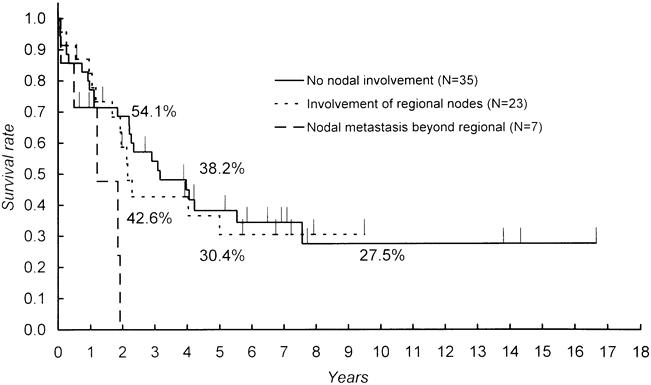
Results: Sixty percent of the patients with resectional surgery had stage IVA or IVB disease, and 92.3% of them underwent major hepatectomies. No in-hospital deaths were encountered in the 35 most recent resections, whereas there were six deaths in the early period. Resectional surgery was associated with a survival benefit, especially when resection margins were free from cancerous infiltration. The estimated 5-year survival rate after resection, including all deaths, was 34.8%; this was 51.6% when the margins were clear. Nodal involvement was documented in 44.6% of the resections. However, patients with metastases limited to the regional nodes showed a survival rate similar to that in patients without nodal involvement. Significant predictive factors for survival after resection were extension to the gallbladder, nodal status, resectional margins, histologic type, and gender.
Conclusions: The combination of major hepatectomy with systematic nodal dissection gave a good chance of prolonged survival for patients with carcinoma involving the hepatic hilus, even when the disease was advanced. Less-extensive procedures were also beneficial for less-advanced disease if clear resectional margins were secured.
Figures
References
-
- Klatskin G. Adenocarcinoma of the hepatic duct at its bifurcation within the porta hepatis: an unusual tumor with distinctive clinical and pathologic features. Am J Med 1965; 38:241–256. - PubMed
-
- Guthrie CM, Haddock G, De Beaux AC, et al. Changing trends in the management of extrahepatic cholangiocarcinoma. Br J Surg 1993; 80:1434–1439. - PubMed
-
- Kuvshinoff BW, Armstrong JG, Fong Y, et al. Palliation of irresectable hilar cholangiocarcinoma with biliary drainage and radiotherapy. Br J Surg 1995; 82:1522–1525. - PubMed
-
- Liu CL, Lo CM, Lai EC, et al. Endoscopic retrograde cholangiopancreatography and endoscopic endoprosthesis insertion in patients with Klatskin tumors. Arch Surg 1998; 133:293–296. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
