

Epidemiology of syncope in hospitalized patients
- PMID: 10571716
- PMCID: PMC1496762
- DOI: 10.1046/j.1525-1497.1999.03199.x
Epidemiology of syncope in hospitalized patients
Abstract
Objective: To describe the etiologies of syncope in hospitalized patients and determine the factors that influence survival after discharge.
Design: Observational retrospective cohort.
Setting: Department of Veterans Affairs hospital, group-model HMO, and Medicare population in Oregon.
Patients: Hospitalized individuals (n = 1,516; mean age +/- SD, 73.0 +/- 13.4 years) with an admission or discharge diagnosis of syncope (ICD-9-CM 780.2) during 1992, 1993, or 1994.
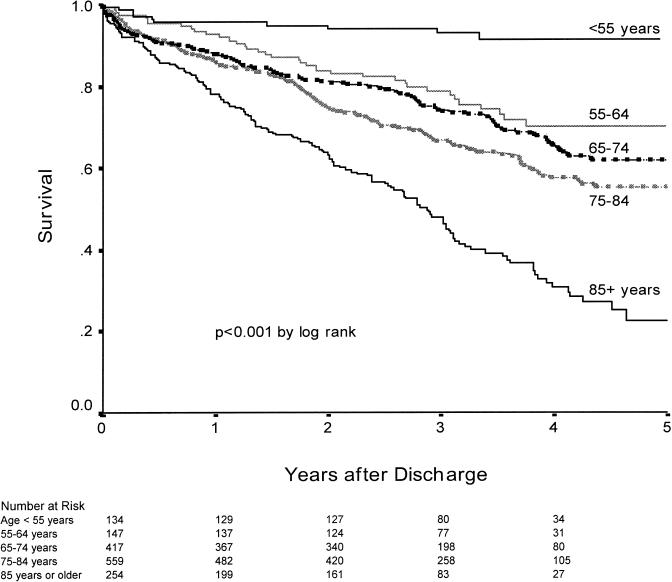
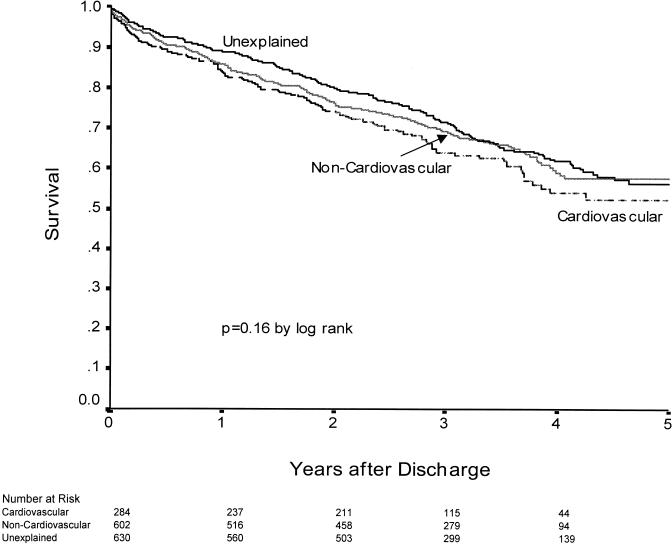
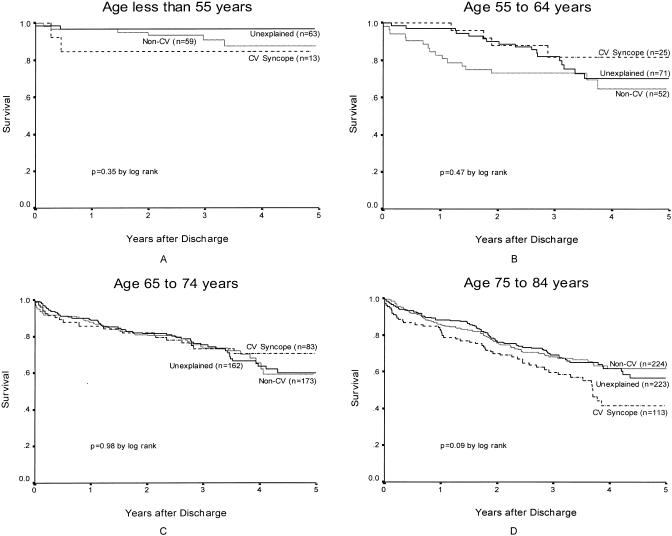
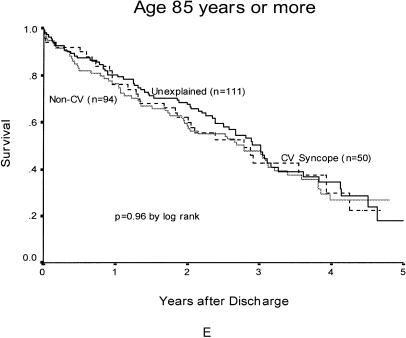
Measurements and main results: During a median hospital stay of 3 days, most individuals received an electrocardiogram (97%) and prolonged electrocardiographic monitoring (90%), but few underwent electrophysiology testing (2%) or tilt-table testing (0. 7%). The treating clinicians identified cardiovascular causes of syncope in 19% of individuals and noncardiovascular causes in 40%. The remaining 42% of individuals were discharged with unexplained syncope. Complete heart block (2.4%) and ventricular tachycardia (2. 3%) were rarely identified as the cause of syncope. Pacemakers were implanted in 28% of the patients with cardiovascular syncope and 0. 4% of the others. No patient received an implantable defibrillator. All-cause mortality +/- SE was 1.1% +/- 0.3% during the admission, 13% +/- 1% at 1 year, and 41% +/- 2% at 4 years. The adjusted relative risk (RR) of dying for individuals with cardiovascular syncope (RR 1.18; 95% confidence interval [CI] 0.92, 1.50) did not differ from that for unexplained syncope (RR 1.0) and noncardiovascular syncope (RR 0.94; 95% CI 0.77, 1.16).
Conclusions: Among these elderly patients hospitalized with syncope, noncardiovascular causes were twice as common as cardiovascular causes. Because survival was not related to the cause of syncope, clinicians cannot be reassured that hospitalized elderly patients with noncardiovascular and unexplained syncope will have excellent outcomes.
Figures
Similar articles
-
A comparison of Medicare fee-for-service and a group-model HMO in the inpatient management and long-term survival of elderly individuals with syncope.Am J Manag Care. 2000 Oct;6(10):1089-98. Am J Manag Care. 2000. PMID: 11184665
-
Clinical Benefit of Hospitalization for Older Adults With Unexplained Syncope: A Propensity-Matched Analysis.Ann Emerg Med. 2019 Aug;74(2):260-269. doi: 10.1016/j.annemergmed.2019.03.031. Epub 2019 May 9. Ann Emerg Med. 2019. PMID: 31080027 Free PMC article.
-
Epidemiological studies on syncope.Dan Med J. 2013 Sep;60(9):B4702. Dan Med J. 2013. PMID: 24001470 Review.
-
Prognosis among healthy individuals discharged with a primary diagnosis of syncope.J Am Coll Cardiol. 2013 Jan 22;61(3):325-32. doi: 10.1016/j.jacc.2012.08.1024. Epub 2012 Dec 12. J Am Coll Cardiol. 2013. PMID: 23246392
-
Epidemiological studies on syncope--a register based approach.Dan Med J. 2013 Aug;60(8):B4702. Dan Med J. 2013. PMID: 24063058 Review.
Cited by
-
Reliability of Clinical Assessments in Older Adults With Syncope or Near Syncope.Acad Emerg Med. 2016 Sep;23(9):1014-21. doi: 10.1111/acem.12977. Epub 2016 Sep 6. Acad Emerg Med. 2016. PMID: 27027730 Free PMC article.
-
The prevalence and prognostic significance of near syncope and syncope: a prospective study of 395 cases in an emergency department (the SPEED study).Dtsch Arztebl Int. 2014 Mar 21;111(12):197-204. doi: 10.3238/arztebl.2014.0197. Dtsch Arztebl Int. 2014. PMID: 24717304 Free PMC article.
-
Patterns and preexisting risk factors of 30-day mortality after a primary discharge diagnosis of syncope or near syncope.Acad Emerg Med. 2012 May;19(5):488-96. doi: 10.1111/j.1553-2712.2012.01336.x. Acad Emerg Med. 2012. PMID: 22594351 Free PMC article.
-
Diagnostic Value of the TpTe Interval in Children with Ventricular Arrhythmias.Int J Environ Res Public Health. 2021 Nov 20;18(22):12194. doi: 10.3390/ijerph182212194. Int J Environ Res Public Health. 2021. PMID: 34831949 Free PMC article.
-
Patients with syncope in a German emergency department: description of patients and processes.Dtsch Arztebl Int. 2012 Jan;109(4):58-65. doi: 10.3238/arztebl.2012.0058. Epub 2012 Jan 27. Dtsch Arztebl Int. 2012. PMID: 22334828 Free PMC article.
References
-
- Kapoor WN. Evaluation and management of the patient with syncope. JAMA. 1992;268:2553–60. - PubMed
-
- Kapoor WN, Karpf M, Wieand S, Peterson JR, Levey GS. A prospective evaluation and follow-up of patients with syncope. N Engl J Med. 1983;309:197–204. - PubMed
-
- Silverstein MD, Singer DE, Mulley AG, Thibault GE, Barnett GO. Patients with syncope admitted to medical intensive care units. JAMA. 1982;248:1185–9. - PubMed
-
- Day SC, Cook EF, Funkenstein H, Goldman L. Evaluation and outcome of emergency room patients with transient loss of consciousness. Am J Med. 1982;73:15–23. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical