

Improving response to critical laboratory results with automation: results of a randomized controlled trial
- PMID: 10579608
- PMCID: PMC61393
- DOI: 10.1136/jamia.1999.0060512
Improving response to critical laboratory results with automation: results of a randomized controlled trial
Abstract
Objective: To evaluate the effect of an automatic alerting system on the time until treatment is ordered for patients with critical laboratory results.
Design: Prospective randomized controlled trial.
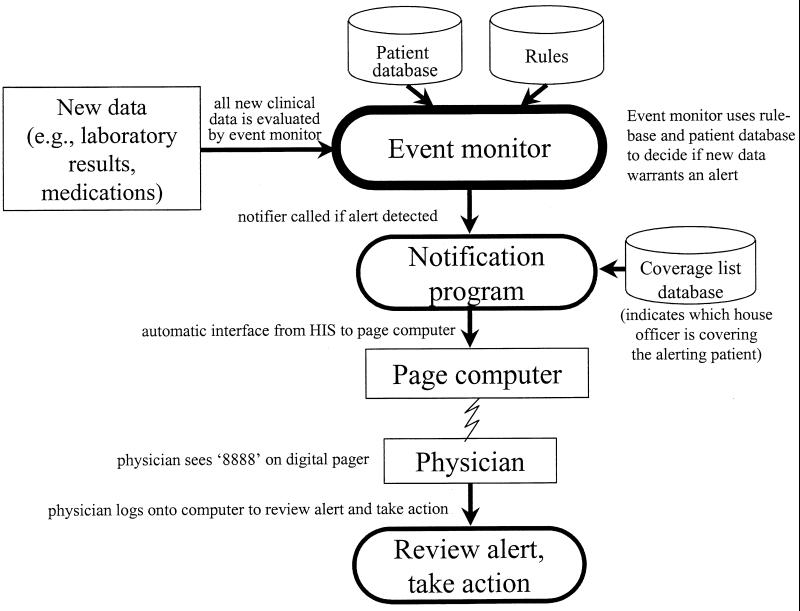
Intervention: A computer system to detect critical conditions and automatically notify the responsible physician via the hospital's paging system.
Patients: Medical and surgical inpatients at a large academic medical center. One two-month study period for each service.
Main outcomes: Interval from when a critical result was available for review until an appropriate treatment was ordered. Secondary outcomes were the time until the critical condition resolved and the frequency of adverse events.
Methods: The alerting system looked for 12 conditions involving laboratory results and medications. For intervention patients, the covering physician was automatically notified about the presence of the results. For control patients, no automatic notification was made. Chart review was performed to determine the outcomes.
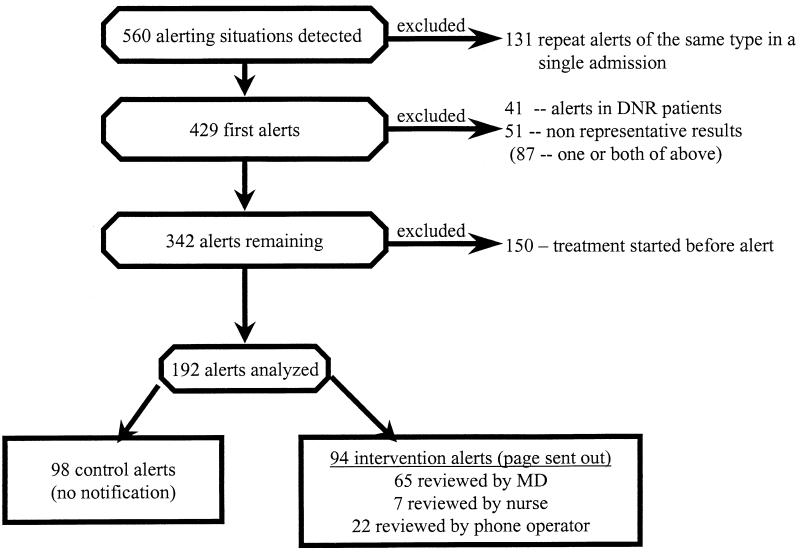
Results: After exclusions, 192 alerting situations (94 interventions, 98 controls) were analyzed. The intervention group had a 38 percent shorter median time interval (1.0 hours vs. 1.6 hours, P = 0.003; mean, 4.1 vs. 4.6 hours, P = 0.003) until an appropriate treatment was ordered. The time until the alerting condition resolved was less in the intervention group (median, 8.4 hours vs. 8.9 hours, P = 0.11; mean, 14.4 hours vs. 20.2 hours, P = 0.11), although these results did not achieve statistical significance. The impact of the intervention was more pronounced for alerts that did not meet the laboratory's critical reporting criteria. There was no significant difference between the two groups in the number of adverse events.
Conclusion: An automatic alerting system reduced the time until an appropriate treatment was ordered for patients who had critical laboratory results. Information technologies that facilitate the transmission of important patient data can potentially improve the quality of care.
Figures
Similar articles
-
How promptly are inpatients treated for critical laboratory results?J Am Med Inform Assoc. 1998 Jan-Feb;5(1):112-9. doi: 10.1136/jamia.1998.0050112. J Am Med Inform Assoc. 1998. PMID: 9452990 Free PMC article.
-
Real-time clinical alerting: effect of an automated paging system on response time to critical laboratory values--a randomised controlled trial.Qual Saf Health Care. 2010 Apr;19(2):99-102. doi: 10.1136/qshc.2008.028407. Qual Saf Health Care. 2010. PMID: 20351157 Clinical Trial.
-
Real-time automated paging and decision support for critical laboratory abnormalities.BMJ Qual Saf. 2011 Nov;20(11):924-30. doi: 10.1136/bmjqs.2010.051110. Epub 2011 Jul 1. BMJ Qual Saf. 2011. PMID: 21725046
-
Safety and Efficacy of Imatinib for Hospitalized Adults with COVID-19: A structured summary of a study protocol for a randomised controlled trial.Trials. 2020 Oct 28;21(1):897. doi: 10.1186/s13063-020-04819-9. Trials. 2020. PMID: 33115543 Free PMC article.
-
Systematic reviews of the effectiveness of day care for people with severe mental disorders: (1) acute day hospital versus admission; (2) vocational rehabilitation; (3) day hospital versus outpatient care.Health Technol Assess. 2001;5(21):1-75. doi: 10.3310/hta5210. Health Technol Assess. 2001. PMID: 11532238 Review.
Cited by
-
Pathogen profiling for disease management and surveillance.Nat Rev Microbiol. 2007 Jun;5(6):464-70. doi: 10.1038/nrmicro1656. Epub 2007 May 8. Nat Rev Microbiol. 2007. PMID: 17487146 Free PMC article. Review.
-
Diagnostic Bacteriology in District Hospitals in Sub-Saharan Africa: At the Forefront of the Containment of Antimicrobial Resistance.Front Med (Lausanne). 2019 Sep 23;6:205. doi: 10.3389/fmed.2019.00205. eCollection 2019. Front Med (Lausanne). 2019. PMID: 31608280 Free PMC article. Review.
-
The use of computers for clinical care: a case series of advanced U.S. sites.J Am Med Inform Assoc. 2003 Jan-Feb;10(1):94-107. doi: 10.1197/jamia.m1127. J Am Med Inform Assoc. 2003. PMID: 12509360 Free PMC article.
-
Understanding Electronic AKI Alerts: Characterization by Definitional Rules.Kidney Int Rep. 2016 Dec 9;2(3):342-349. doi: 10.1016/j.ekir.2016.12.001. eCollection 2017 May. Kidney Int Rep. 2016. PMID: 29142963 Free PMC article.
-
Not if but when; no longer why but how.Crit Care. 2007;11(1):117. doi: 10.1186/cc5688. Crit Care. 2007. PMID: 17328788 Free PMC article.
References
-
- Leape LL. Error in medicine. JAMA 1994:272(23);1851-7. - PubMed
-
- Bedell SE, Deitz DC, Leeman D, Delbanco TL. Incidence and characteristics of preventable iatrogenic cardiac arrests. JAMA. 1991;265(21):2815-20. - PubMed
-
- Leape LL, Bates DW, Cullen DJ, et al. Systems analysis of adverse drug events. ADE Prevention Study Group. JAMA. 1995;274(1):35-43. - PubMed
-
- Classen DC, Evans RS, Pestotnik SL, Horn SD, Menlove RL, Burke JP. The timing of prophylactic administration of antibiotics and the risk of surgical-wound infection. N Engl J Med. 1992;326(5):281-6. - PubMed
-
- Classen DC. Clinical decision support systems to improve clinical practice and quality of care. JAMA. 1998;280(15):1360-1. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
