

Development of the biologically active Guglielmi detachable coil for the treatment of cerebral aneurysms. Part II: an experimental study in a swine aneurysm model
- PMID: 10588133
- PMCID: PMC7657805
Development of the biologically active Guglielmi detachable coil for the treatment of cerebral aneurysms. Part II: an experimental study in a swine aneurysm model
Abstract
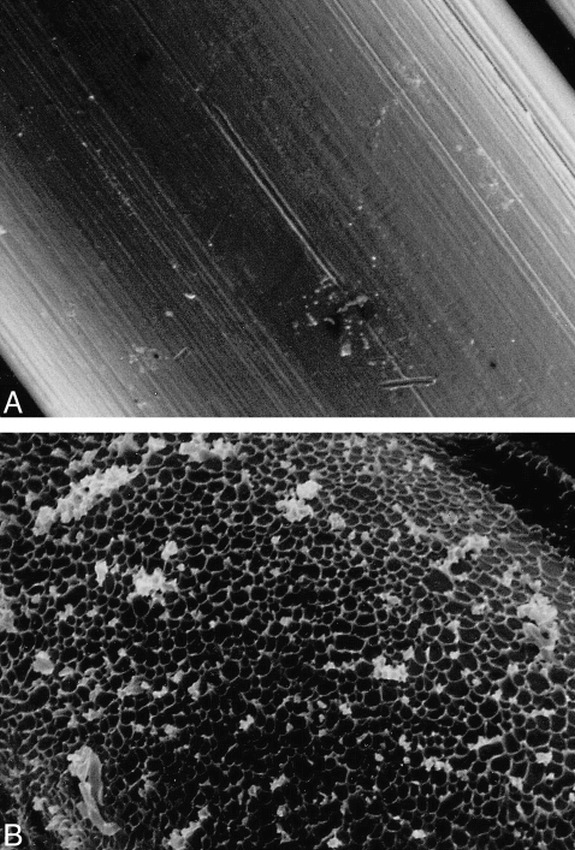
Background and purpose: Ion implantation is a surface-modification technology that creates a borderless surface on protein-coated platinum; this change in physical and chemical properties on the surface of Guglielmi detachable coils (GDCs) appears to enhance cell proliferation and adhesion. Our purpose was to evaluate the effect of ion implantation on GDCs in an experimental aneurysm model.
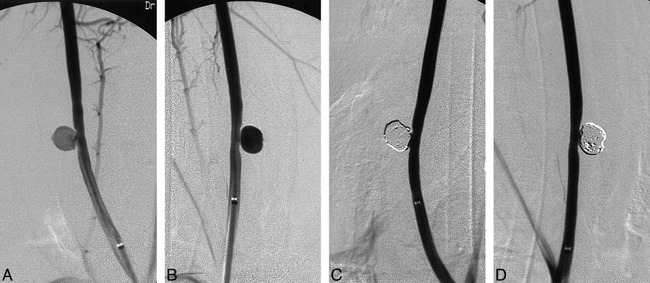
Methods: GDCs were coated with either type I collagen, fibronectin, vitronectin, laminin, or fibrinogen. Using He+ or Ne+ 1 x 10(14-15) ions/cm2, ion implantation was performed on these protein-coated GDCs (GDC-Is). A total of 56 experimental aneurysms were constructed microsurgically in the common carotid arteries of 28 swine. These experimental aneurysms were embolized with standard GDCs (n = 23), collagen GDC-Is (n = 11), vitronectin GDC-Is (n = 6), laminin GDC-Is (n = 4), fibrinogen GDC-Is (n = 6), and fibronectin GDC-Is (n = 6). The animals were sacrificed at day 14 after coil embolization. The physical properties of the new coils (friction on delivery, deployment into aneurysms, trackability, etc) and the development of tissue scarring and neoendothelium across the aneurysm's orifice were evaluated macroscopically and microscopically.
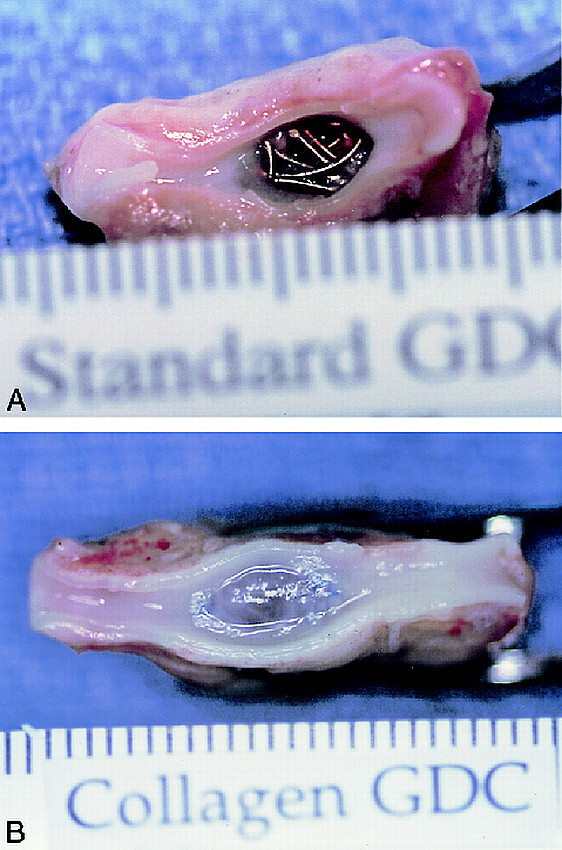
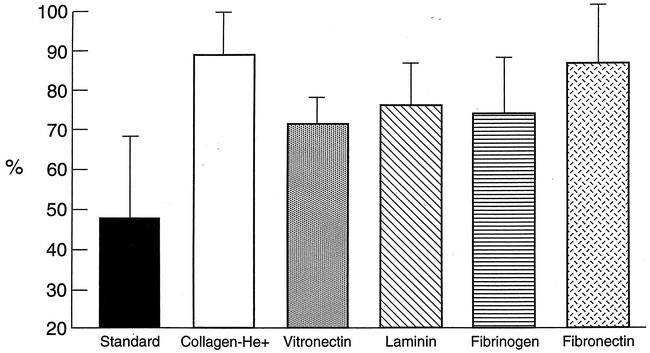
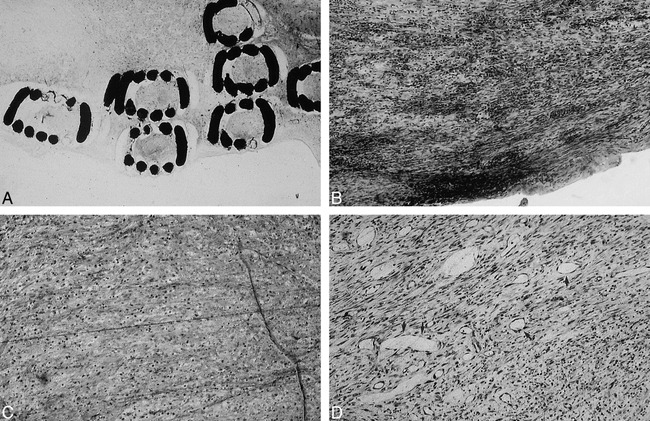
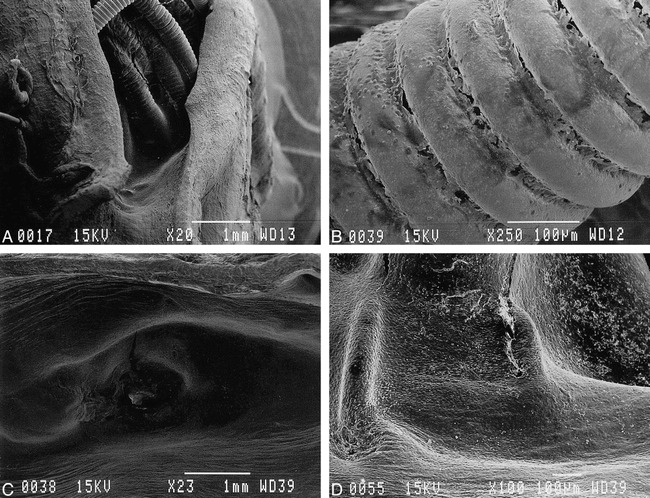
Results: No evidence of increased coil friction/stiffness was observed during delivery of GDC-Is through microcatheters in this aneurysm model. A more intense scar formation and neoendothelium at the neck of aneurysms were observed macroscopically when treated with GDC-Is. Significant differences in the proportion of neck coverage between standard GDCs (48.3% +/- 20.5%) and all GDC-I groups were observed (collagen GDC-I-89.4% +/- 14.9%, P < .01; vitronectin GDC-I-71.5% +/- 7.0%, P < .05; laminin GDC-I-76.5% +/- 11.0%, P < .05; fibrinogen GDC-I-74.8% +/- 13.9%, P < .05; fibronectin GDC-I-87.5% +/- 15.0%, P < .01). Light microscopy showed a well-organized fibrous tissue bridging the aneurysm's neck when using GDC-Is, whereas only a fibrin-like thin layer covered the standard GDC surfaces.
Conclusion: GDC-Is indicated a more intense inflammatory response in the aneurysm body and dome and faster re-endothelial coverage of the neck of the aneurysm. This accelerated histologic response may decrease the chances of coil compaction and aneurysm recanalization. This technology may improve anatomic and clinical outcomes in patients harboring intracranial aneurysms.
Figures
Similar articles
-
Ion implantation and protein coating of detachable coils for endovascular treatment of cerebral aneurysms: concepts and preliminary results in swine models.Neurosurgery. 1997 Jun;40(6):1233-43; discussion 1243-4. doi: 10.1097/00006123-199706000-00024. Neurosurgery. 1997. PMID: 9179897
-
Hydroxyapatite coating of detachable coils for endovascular occlusion of experimental aneurysm.Interv Neuroradiol. 2001 Dec 22;7(Suppl 1):105-10. doi: 10.1177/15910199010070S115. Epub 2002 Jan 10. Interv Neuroradiol. 2001. PMID: 20663386 Free PMC article.
-
Development of a biologically active Guglielmi detachable coil for the treatment of cerebral aneurysms. Part I: in vitro study.AJNR Am J Neuroradiol. 1999 Nov-Dec;20(10):1986-91. AJNR Am J Neuroradiol. 1999. PMID: 10588132 Free PMC article.
-
Selection of cerebral aneurysms for treatment using Guglielmi detachable coils: the preliminary University of Illinois at Chicago experience.Neurosurgery. 1998 Dec;43(6):1281-95; discussion 1296-7. doi: 10.1097/00006123-199812000-00011. Neurosurgery. 1998. PMID: 9848841 Review.
-
Acute human histopathology of an intracranial aneurysm treated using Guglielmi detachable coils: case report and review of the literature.Neurosurgery. 1998 Nov;43(5):1203-8. doi: 10.1097/00006123-199811000-00106. Neurosurgery. 1998. PMID: 9802864 Review.
Cited by
-
Common swine models of cardiovascular disease for research and training.Lab Anim (NY). 2016 Feb;45(2):67-74. doi: 10.1038/laban.935. Lab Anim (NY). 2016. PMID: 26814353
-
Interval change in size of venous pouch canine bifurcation aneurysms over a 10-month period.AJNR Am J Neuroradiol. 2008 Jun;29(6):1067-70. doi: 10.3174/ajnr.A1046. Epub 2008 Apr 3. AJNR Am J Neuroradiol. 2008. PMID: 18388214 Free PMC article.
-
Monitoring of the heparinization in the rabbit animal model during endovascular interventions.Neuroradiology. 2013 Jul;55(7):883-8. doi: 10.1007/s00234-013-1189-y. Epub 2013 Apr 26. Neuroradiology. 2013. PMID: 23619701
-
Comparison of platinum and first-generation Matrix coils in under-packed canine side-wall aneurysms: evaluation of progressive thrombosis.Neuroradiology. 2007 Nov;49(11):939-45. doi: 10.1007/s00234-007-0280-7. Epub 2007 Aug 16. Neuroradiology. 2007. PMID: 17701406
-
Experimental polyvinyl alcohol core coil for a drug delivery system.Interv Neuroradiol. 2003 May 15;9(Suppl 1):107-11. doi: 10.1177/15910199030090S114. Epub 2004 Oct 22. Interv Neuroradiol. 2003. PMID: 20591238 Free PMC article.
References
-
- Guglielmi G, Viñuela F, Dion J, Duckwiler G, Electrothrombosis of saccular aneurysms via endovascular approach: Part 2-preliminary clinical experience. J Neurosurg 1991;75:8-14 - PubMed
-
- Guglielmi G, Viñuela F, Duckwiler G, et al. Endovascular treatment of posterior circulation aneurysms by electrothrombosis using electrically detachable coils. J Neurosurg 1992;77:515-524 - PubMed
-
- Murayama Y, Malisch T, Guglielmi G, et al. Incidence of cerebral vasospasm after endovascular treatment of acutely ruptured aneurysms: report on 69 cases. J Neurosurg 1997;87:830-835 - PubMed
-
- Murayama Y, Viñuela F, Duckwiler GR, Gobin YP, Guglielmi G, Embolization of incidental cerebral aneurysms by using the Guglielmi detachable coil system. J Neurosurg 1999;90:207-214 - PubMed
-
- Viñuela F, Duckwiler G, Mawad M, Guglielmi detachable coil embolization of acute intracranial aneurysm: perioperative anatomical and clinical outcome in 403 patients. J Neurosurg 1997;86:475-482 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical