

Determinants of resource utilization in the treatment of brain arteriovenous malformations
- PMID: 10588135
- PMCID: PMC7657781
Determinants of resource utilization in the treatment of brain arteriovenous malformations
Abstract
Background and purpose: Preoperative embolization of arteriovenous malformations (AVMs) is thought to improve outcome following surgical resection of these lesions. The purpose of this study was to examine the cost associated with preoperative embolization and different surgical risk categories in the surgical treatment of brain AVMs.
Methods: In a review of 126 patients treated surgically for resection of AVMs, we noted the total days spent in the hospital and calculated the associated costs (from hospital and estimated professional fees). Surgical risk category was determined using the Spetzler-Martin grading system. We examined the effect of risk category, preoperative embolization, and outcome (Rankin score) on cost and inpatient days.
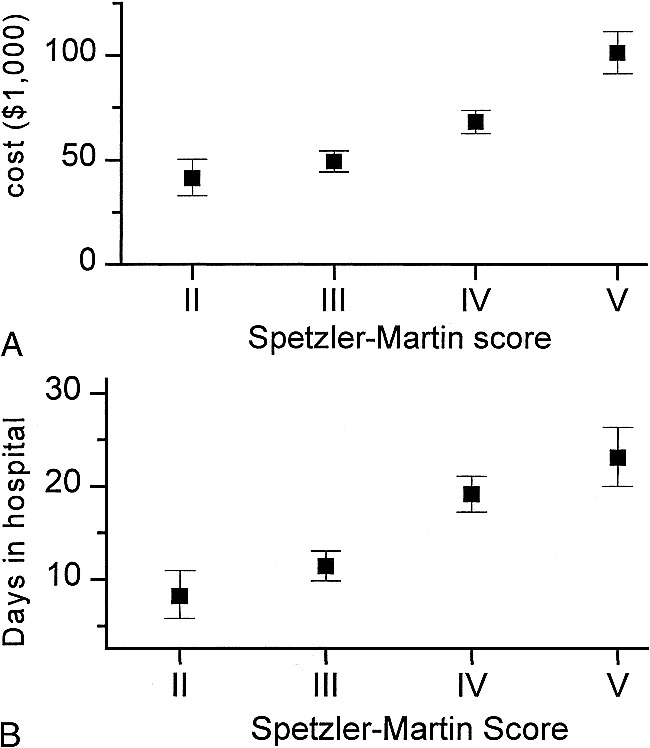
Results: Preoperative embolization and greater surgical risk were independently associated with higher total costs. Average adjusted cost for embolization and surgery was $78,400 +/- $4,900 versus $49,300 +/- $5,800 for surgery alone. Patients ranged in preoperative risk category from Spetzler-Martin grades II through V, with an average increase of $20,100 in total cost per Spetzler-Martin grade (95% CI, $13,500 to $28,100). Higher surgical risk category was also associated with more days spent in hospital, with an average increase of 6 days per increment in Spetzler-Martin grade (95% CI, 4 to 8). After surgical resection of an AVM, new neurologic deficits were associated with large differences in cost: $68,500 +/- $6,100 and 15 +/- 2 days in hospital for patients who were neurologically worse after surgery, versus $44,700 +/- $3,900 and 10 +/- 1 days for patients who were unchanged.
Conclusion: Preoperative embolization in the treatment of AVMs is associated with higher cost but not more days in the hospital. Patients with higher Spetzler-Martin grade AVMs utilize more hospital resources, in part because they have poorer neurologic outcome, and postoperative deficits are associated with higher costs and more days in the hospital.
Figures

Similar articles
-
Microsurgery for cerebral arteriovenous malformations: subgroup outcomes in a consecutive series of 288 cases.J Neurosurg. 2017 Apr;126(4):1056-1063. doi: 10.3171/2016.4.JNS153017. Epub 2016 Jun 10. J Neurosurg. 2017. PMID: 27285541 Clinical Trial.
-
Onyx Embolization Before the Surgical Treatment of Grade III Spetzler-Martin Brain Arteriovenous Malformations: Single-Center Experience and Technical Nuances.World Neurosurg. 2018 Aug;116:e340-e353. doi: 10.1016/j.wneu.2018.04.203. Epub 2018 May 9. World Neurosurg. 2018. PMID: 29751183
-
Multimodality treatment of cerebral arteriovenous malformations.World Neurosurg. 2014 Jul-Aug;82(1-2):149-59. doi: 10.1016/j.wneu.2013.02.064. Epub 2013 Feb 20. World Neurosurg. 2014. PMID: 23454686
-
[Current management of arteriovenous malformations. Retrospective study of 31 cases and literature review].Neurocirugia (Astur). 2007 Oct;18(5):394-404; discussion 404-5. Neurocirugia (Astur). 2007. PMID: 18008013 Review. Spanish.
-
Surgical treatment of intracranial arteriovenous malformations with an analysis of cost-effectiveness.Clin Neurosurg. 1995;42:348-69. Clin Neurosurg. 1995. PMID: 8846602 Review.
Cited by
-
Cost determinants in management of brain arteriovenous malformations.Acta Neurochir (Wien). 2020 Jan;162(1):169-173. doi: 10.1007/s00701-019-04134-6. Epub 2019 Nov 23. Acta Neurochir (Wien). 2020. PMID: 31760534 Free PMC article.
-
Diagnosis and treatment of arteriovenous malformations.Curr Neurol Neurosci Rep. 2013 Feb;13(2):324. doi: 10.1007/s11910-012-0324-1. Curr Neurol Neurosci Rep. 2013. PMID: 23307509 Review.
-
Management of unbled brain arteriovenous malformation study.Neurol Clin. 2015 May;33(2):347-59. doi: 10.1016/j.ncl.2014.12.006. Neurol Clin. 2015. PMID: 25907910 Free PMC article. Review.
-
Treatment of arteriovenous malformations of the brain.Curr Neurol Neurosci Rep. 2007 Jan;7(1):28-34. doi: 10.1007/s11910-007-0018-2. Curr Neurol Neurosci Rep. 2007. PMID: 17217851 Review.
-
Viewpoints on the ARUBA trial.AJNR Am J Neuroradiol. 2015 Apr;36(4):615-7. doi: 10.3174/ajnr.A4204. Epub 2014 Dec 26. AJNR Am J Neuroradiol. 2015. PMID: 25542877 Free PMC article. No abstract available.
References
-
- Brown RD, Jr, Wiebers DO, Torner JC, O'Fallon WM, Frequency of intracranial hemorrhage as a presenting symptom and subtype analysis: a population-based study of intracranial vascular malformations in Olmsted County, Minnesota. J Neurosurg 1996;85:29-32 - PubMed
-
- Ostfeld AM, A review of stroke epidemiology. Epidemiol Rev 1980;2:136-152 - PubMed
-
- Brown RD, Jr, Wiebers DO, Forbes G, et al. The natural history of unruptured intracranial arteriovenous malformations. J Neurosurg 1988;68:352-357 - PubMed
-
- Graf CJ, Perret GE, Torner JC, Bleeding from cerebral arteriovenous malformations as part of their natural history. J Neurosurg 1983;58:331-337 - PubMed
-
- Ondra SL, Troupp H, George ED, Schwab K, The natural history of symptomatic arteriovenous malformations of the brain: a 24-year follow-up assessment. J Neurosurg 1990;73:387-391 - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources