

Clonal expansion and loss of heterozygosity at chromosomes 9p and 17p in premalignant esophageal (Barrett's) tissue
- PMID: 10601379
- PMCID: PMC1559996
- DOI: 10.1093/jnci/91.24.2087
Clonal expansion and loss of heterozygosity at chromosomes 9p and 17p in premalignant esophageal (Barrett's) tissue
Abstract
Background: Abnormalities involving the p16 (also known as cyclin-dependent kinase N2 [CDKN2], p16 [INK4a], or MTS1) and p53 (also known as TP53) tumor suppressor genes are highly prevalent in esophageal adenocarcinomas. Loss of heterozygosity (LOH) at 9p21 and 17p13 chromosomes (locations for p16 and p53 genes, respectively) is frequently observed in the premalignant condition, Barrett's esophagus. We studied extensively the distribution and heterogeneity of LOH at 9p and 17p chromosomes throughout the Barrett's segment in patients who have not yet developed esophageal adenocarcinoma.
Methods: We evaluated 404 samples from 61 consecutive patients enrolled in the Seattle Barrett's Esophagus Study from February 1995 through September 1998. All patients had high-grade dysplasia but no diagnosis of cancer. The samples were assayed for LOH at 9p and 17p chromosomes after amplification of genomic DNA by use of polymerase chain reaction and DNA genotyping. The cell fractions were purified by flow cytometry on the basis of DNA content and proliferation-associated antigen labeling. Association between LOH at 9p and LOH at 17p with flow cytometric abnormalities was determined by chi-squared test, and logistic regression models were used to model and test for the extent to which a particular genotype was found in 2-cm intervals.
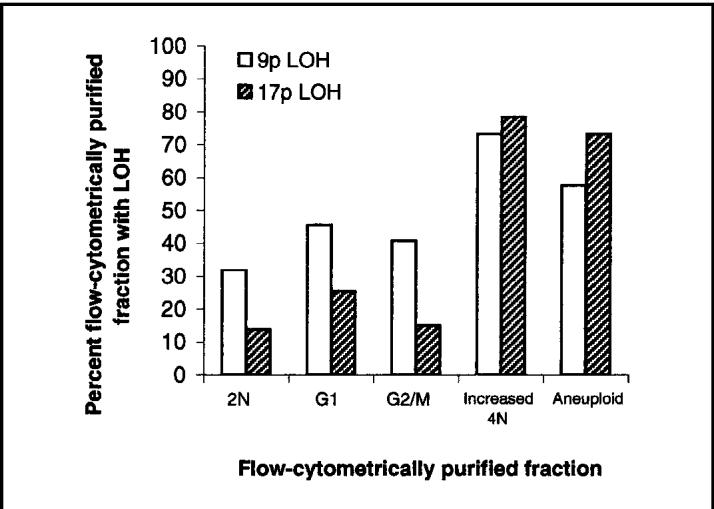
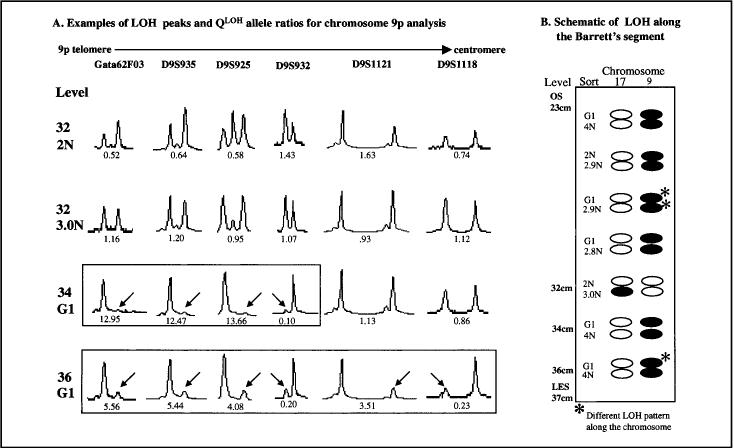
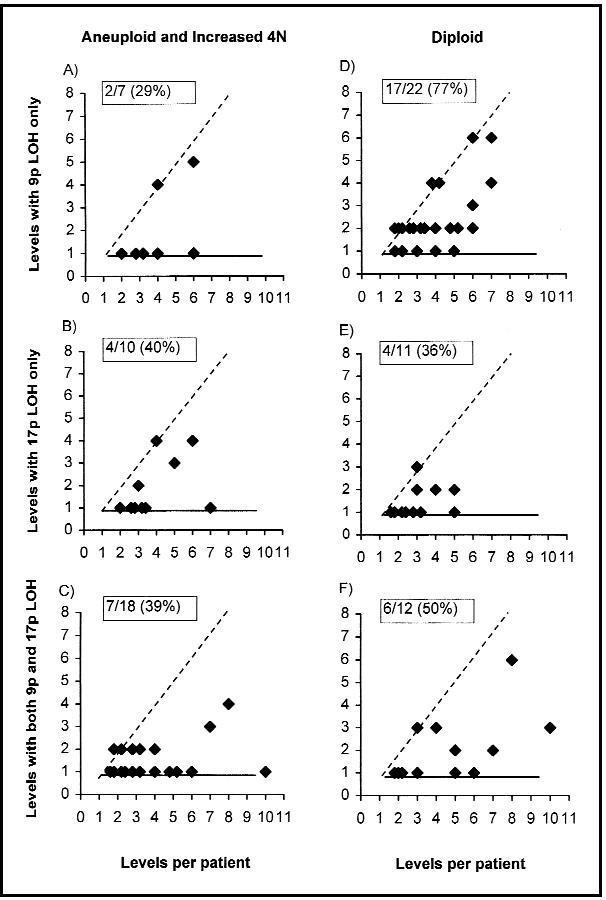
Results and conclusions: LOH at 9p and 17p chromosomes are highly prevalent somatic genetic lesions in premalignant Barrett's tissue. LOH at 9p is more common than LOH at 17p in diploid samples and can be detected over greater regions of Barrett's epithelium. In most patients with high-grade dysplasia, the Barrett's mucosa contains a mosaic of clones and subclones with different patterns of LOH. Some clones had expanded to involve extensive regions of Barrett's epithelium. LOH at 9p and 17p chromosomes may be useful biomarkers to stratify patients' risk of progression to esophageal cancer.
Figures

References
-
- Phillips RW, Wong RK. Barrett’s esophagus. Natural history, incidence, etiology, and complications. Gastroenterol Clin North Am. 1991;20:791–816. - PubMed
-
- Reid BJ. Barrett’s esophagus and esophageal adenocarcinoma. Gastroenterol Clin North Am. 1991;20:817–34. - PubMed
-
- Blot WJ, Devesa SS, Kneller RW, Fraumeni JF., Jr. Rising incidence of adenocarcinoma of the esophagus and gastric cardia. JAMA. 1991;265:1287–9. - PubMed
-
- Powell J, McConkey CC. The rising trend in oesophageal adenocarcinoma and gastric cardia. Eur J Cancer Prev. 1992;1:265–9. - PubMed
-
- Devesa SS, Blot WJ, Fraumeni JF., Jr. Changing patterns in the incidence of esophageal and gastric carcinoma in the United States. Cancer. 1998;83:2049–53. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
