

Ileoneorectal anastomosis: early clinical results of a restorative procedure for ulcerative colitis and familial adenomatous polyposis without formation of an ileoanal pouch
- PMID: 10615929
- PMCID: PMC1420938
- DOI: 10.1097/00000658-199912000-00003
Ileoneorectal anastomosis: early clinical results of a restorative procedure for ulcerative colitis and familial adenomatous polyposis without formation of an ileoanal pouch
Abstract
Objective: To evaluate a new surgical procedure, ileoneorectal anastomosis (INRA), in patients with ulcerative colitis (UC) and familial adenomatous polyposis (FAP).
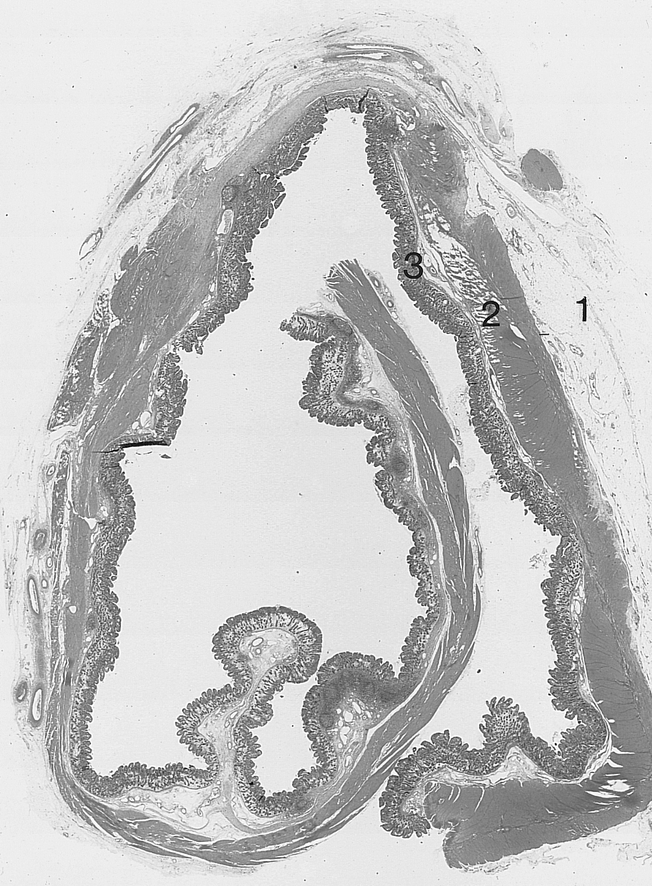
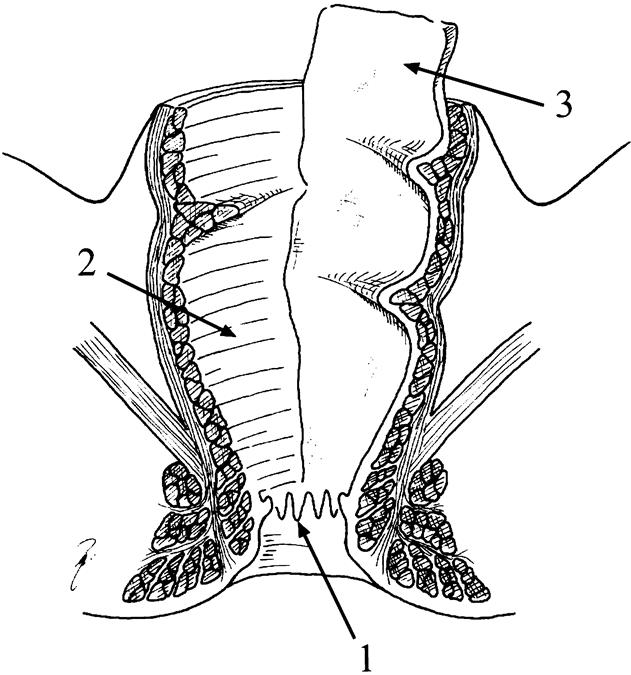
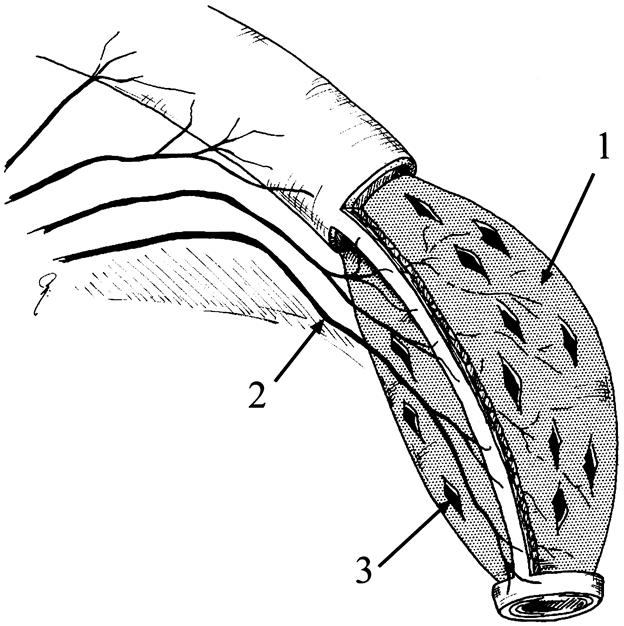
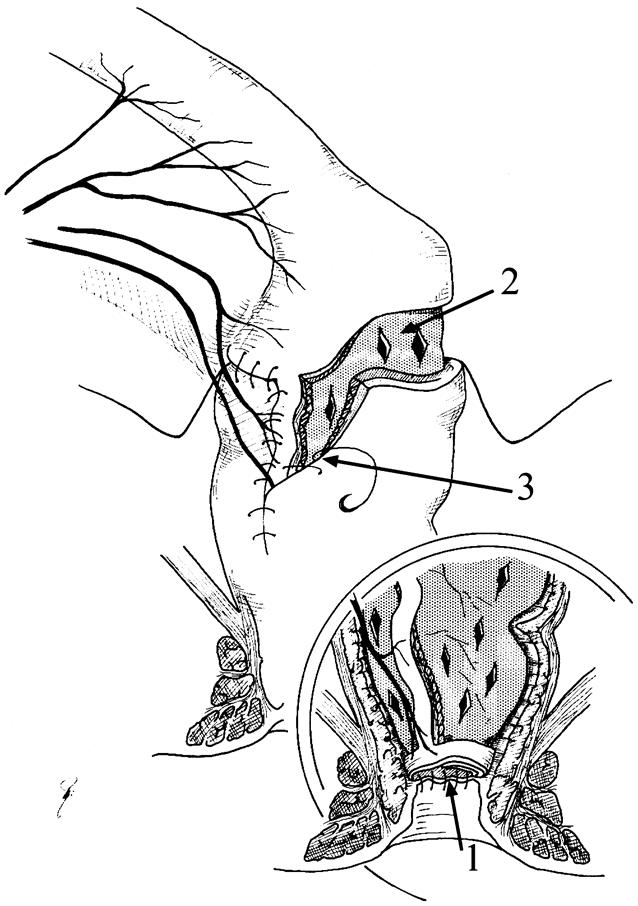
Summary background data: Surgical treatment in UC and FAP aims to resect diseased colonic mucosa and restore oroanal continuity. The ileopouch anal anastomosis achieves this but has a 15% to 35% complication rate, a 10% failure rate, and an unpredictable functional outcome. An alternative surgical technique, INRA, has been developed in which the rectal mucosa is replaced by a vascularized ileal mucosa graft.
Methods: Eleven patients underwent an INRA procedure with a temporary diverting ileostomy. Clinical history, repeat endoscopy, histologic examination, and rectal compliance measurements were carried out before and after surgery.
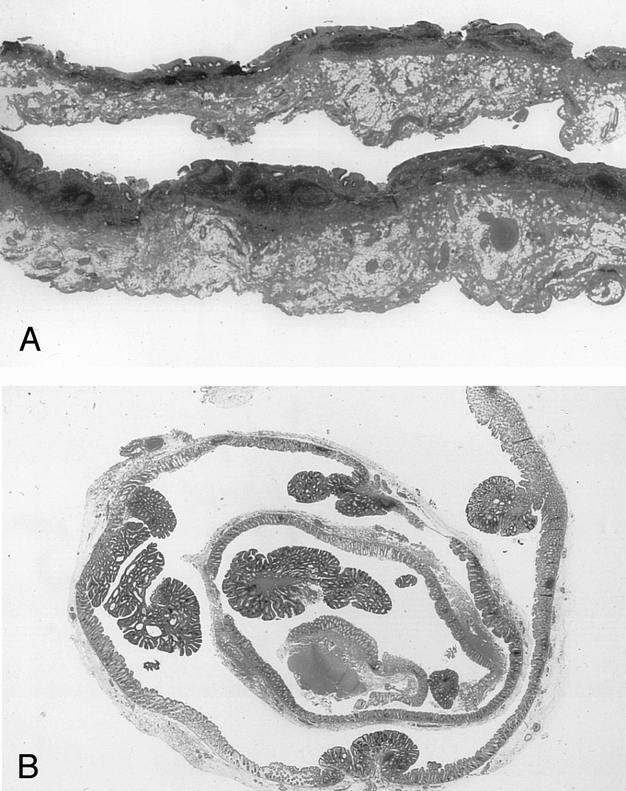
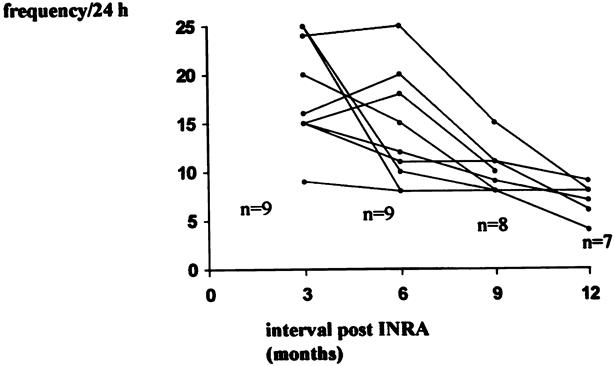
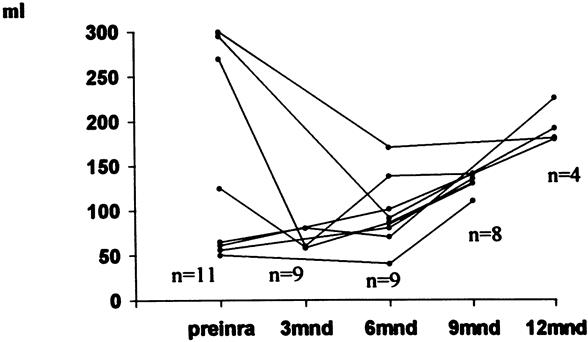
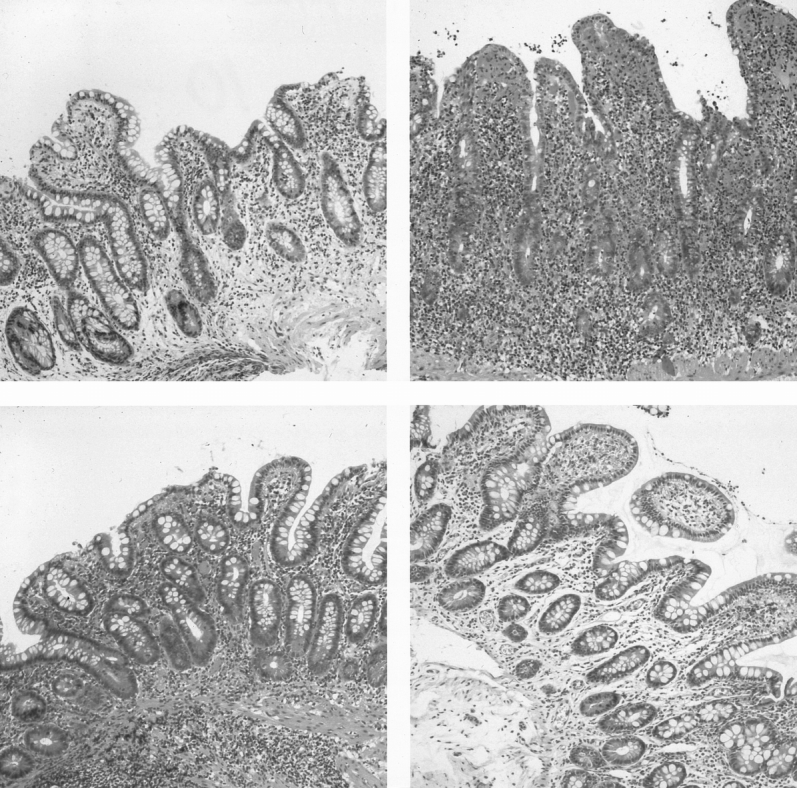
Results: The INRA procedure was technically successful in all patients. Endoscopy showed ingrowth of ileal mucosa in the neorectum, with 100% coverage after 6 weeks. No patient had pelvic sepsis, neorectal-anal or -vaginal fistula, autonomic nerve damage, or fecal incontinence. Neorectal function improved with time. The median 24-hour defecation frequency decreased from 15 (range 9 to 25) to 7 (range 4 to 10) at 11 months follow-up, and the median maximum tolerated volume increased to 157 (range 130 to 225) ml. Anal manometry and electrosensitivity were not affected by the surgery. Histologic biopsy samples after 1 year showed a normal small intestinal mucous membrane, without inflammation or fibrosis.
Conclusion: The combination of a low complication rate and good neorectal function at 1 year is a substantial improvement that justifies extension of the clinical application in patients with UC and FAP.
Figures

Similar articles
-
The ileo neo rectal anastomosis: long-term results of surgical innovation in patients after ulcerative colitis and familial adenomatous polyposis.Int J Colorectal Dis. 2013 Jan;28(1):111-8. doi: 10.1007/s00384-012-1545-0. Epub 2012 Aug 12. Int J Colorectal Dis. 2013. PMID: 22885881 Clinical Trial.
-
Functional outcome of conversion of ileorectal anastomosis to ileal pouch-anal anastomosis in patients with familial adenomatous polyposis and ulcerative colitis.Dis Colon Rectum. 1999 Jul;42(7):903-8. doi: 10.1007/BF02237099. Dis Colon Rectum. 1999. PMID: 10411437
-
[Surgical treatment of ulcerative colitis and familial adenomatous polyposis: recent developments].Ned Tijdschr Geneeskd. 1999 Mar 27;143(13):662-6. Ned Tijdschr Geneeskd. 1999. PMID: 10321297 Review. Dutch.
-
[Application of ileal D-pouch anal anastomosis in the treatment of ulcerative colitis and familial adenomatous polyposis].Zhonghua Wei Chang Wai Ke Za Zhi. 2015 Dec;18(12):1231-4. Zhonghua Wei Chang Wai Ke Za Zhi. 2015. PMID: 26704005 Chinese.
-
[Differential indications for ileoanal pouch anastomosis : Ulcerative colitis, familial adenomatous polyposis, synchronous colorectal cancer - Crohn's disease, constipation].Chirurg. 2017 Jul;88(7):555-558. doi: 10.1007/s00104-017-0421-4. Chirurg. 2017. PMID: 28405717 Review. German.
Cited by
-
The ileo neo rectal anastomosis: long-term results of surgical innovation in patients after ulcerative colitis and familial adenomatous polyposis.Int J Colorectal Dis. 2013 Jan;28(1):111-8. doi: 10.1007/s00384-012-1545-0. Epub 2012 Aug 12. Int J Colorectal Dis. 2013. PMID: 22885881 Clinical Trial.
-
Sexual function and continence after ileo pouch anal anastomosis: a comparison between a meta-analysis and a questionnaire survey.Int J Colorectal Dis. 2004 May;19(3):215-8. doi: 10.1007/s00384-003-0543-7. Epub 2003 Oct 16. Int J Colorectal Dis. 2004. PMID: 14564464
-
Functional results and visceral perception after ileo neo-rectal anastomosis in patients: a pilot study.Gut. 2001 May;48(5):683-9. doi: 10.1136/gut.48.5.683. Gut. 2001. PMID: 11302969 Free PMC article.
-
Assessments of anal canal sensitivity in patients with soiling 5 years or more after colectomy, mucosal proctectomy, and ileal J pouch-anal anastomosis for ulcerative colitis.World J Surg. 2007 Jan;31(1):210-6. doi: 10.1007/s00268-006-0022-8. World J Surg. 2007. PMID: 17180565
References
-
- Wexner SD, Wong WD, Rothenberger DA, Goldberg SM. The ileo-anal reservoir. Am J Surg 1990; 159: 178–185. - PubMed
-
- Meagher AP, Farouk R, Dozois RR, et al. Ileal pouch-anal anastomosis for chronic ulcerative colitis: complications and long-term outcome in 1310 patients. Br J Surg 1998; 85: 800–803. - PubMed
-
- Nicholls RJ. Restorative proctocolectomy with various types of reservoir. World J Surg 1987; 11: 751–762. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
