

Update on meningococcal disease with emphasis on pathogenesis and clinical management
- PMID: 10627495
- PMCID: PMC88937
- DOI: 10.1128/CMR.13.1.144
Update on meningococcal disease with emphasis on pathogenesis and clinical management
Abstract
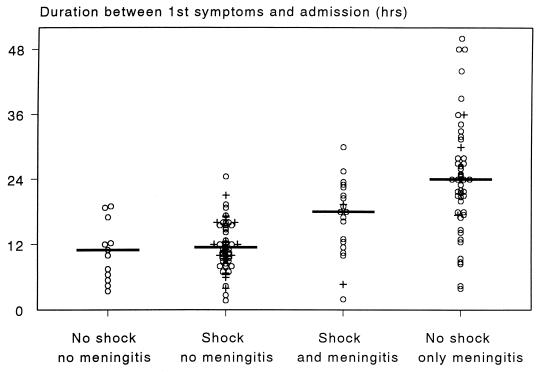
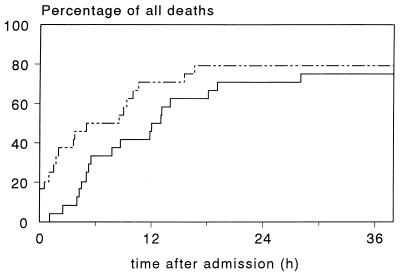
The only natural reservoir of Neisseria meningitidis is the human nasopharyngeal mucosa. Depending on age, climate, country, socioeconomic status, and other factors, approximately 10% of the human population harbors meningococci in the nose. However, invasive disease is relatively rare, as it occurs only when the following conditions are fulfilled: (i) contact with a virulent strain, (ii) colonization by that strain, (iii) penetration of the bacterium through the mucosa, and (iv) survival and eventually outgrowth of the meningococcus in the bloodstream. When the meningococcus has reached the bloodstream and specific antibodies are absent, as is the case for young children or after introduction of a new strain in a population, the ultimate outgrowth depends on the efficacy of the innate immune response. Massive outgrowth leads within 12 h to fulminant meningococcal sepsis (FMS), characterized by high intravascular concentrations of endotoxin that set free high concentrations of proinflammatory mediators. These mediators belonging to the complement system, the contact system, the fibrinolytic system, and the cytokine system induce shock and diffuse intravascular coagulation. FMS can be fatal within 24 h, often before signs of meningitis have developed. In spite of the increasing possibilities for treatment in intensive care units, the mortality rate of FMS is still 30%. When the outgrowth of meningococci in the bloodstream is impeded, seeding of bacteria in the subarachnoidal compartment may lead to overt meningitis within 24 to 36 h. With appropriate antibiotics and good clinical surveillance, the mortality rate of this form of invasive disease is 1 to 2%. The overall mortality rate of meningococcal disease can only be reduced when patients without meningitis, i.e., those who may develop FMS, are recognized early. This means that the fundamental nature of the disease as a meningococcus septicemia deserves more attention.
Figures
References
-
- Abramson J S, Spika J S. Persistence of Neisseria meningitidis in the upper respiratory tract after intravenous antibiotic therapy for systemic meningococcal disease. J Infect Dis. 1985;151:370–371. - PubMed
-
- Achtman M. Global epidemiology of meningococcal disease. In: Cartwright K, editor. Meningococcal disease. Chichester, United Kingdom: John Wiley & Sons, Ltd.; 1995. pp. 159–175.
-
- Achtman M, Wall R A, Bopp M, Kusecek B, Morelli G, Saken E, Hassan King M. Variation in class 5 protein expression by serogroup A meningococci during a meningitis epidemic. J Infect Dis. 1991;164:375–382. - PubMed
-
- Aiuto L T, Barone S R, Cohen P S, Boxer R A. Recombinant tissue plasminogen activator restores perfusion in meningococcal purpura fulminans. Crit Care Med. 1997;25:1079–1082. - PubMed
-
- Algren J T, Lal S, Cutliff S A, Richman B J. Predictors of outcome in acute meningococcal infection in children. Crit Care Med. 1993;21:447–452. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
