

Presence of sorbin in human digestive tract and endocrine digestive tumours
- PMID: 10644311
- PMCID: PMC1727812
- DOI: 10.1136/gut.46.2.182
Presence of sorbin in human digestive tract and endocrine digestive tumours
Abstract
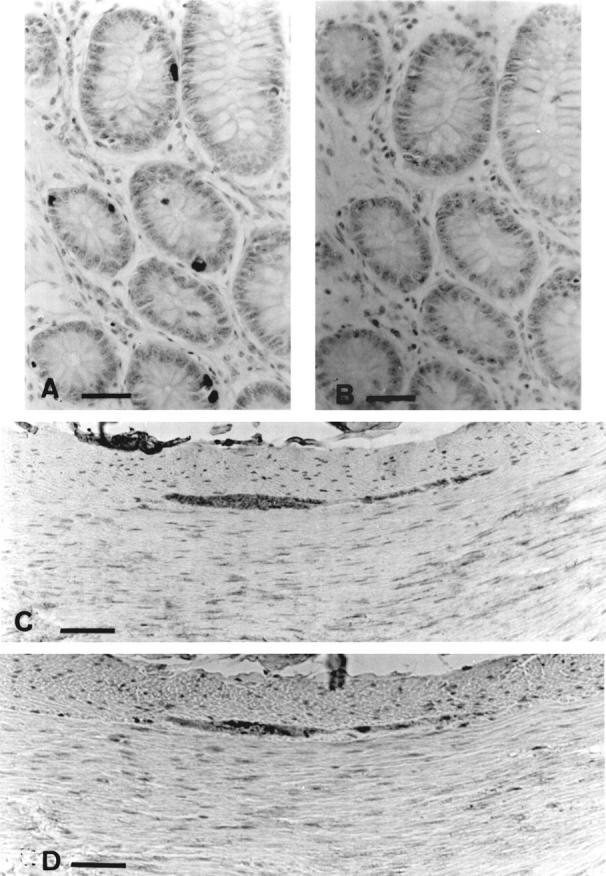
Background: Sorbin, a 153 amino acid peptide isolated from porcine intestine, was localised by immunohistochemistry in endocrine cells of the intestinal mucosa and pancreas and in the enteric nervous system in the pig.
Aims: To identify sorbin cells in normal human digestive tissues and to explore the expression of sorbin in 37 digestive endocrine tumours: 14 intestinal carcinoid tumours and 23 endocrine pancreatic tumours including six insulinomas.
Methods: Two polyclonal antibodies against the C-terminal and the N-terminal sequences of porcine sorbin raised in rabbit were used to evaluate sorbin expression by immunohistochemistry.
Results: In the human digestive tract, sorbin, characterised by both C-terminal and N-terminal immunoreactivity, was found in enterochromaffin cells of the gastric and intestinal epithelium from the pyloric junction to the descending colon. C-Terminal sorbin immunoreactivity alone was found in plexii from the enteric nervous system and in some insulin-containing cells of normal pancreas. C-Terminal and N-terminal antibodies disclosed sorbin in five of 14 intestinal carcinoid tumours; C-terminal antibody alone disclosed a C-terminal sorbin peptide in two of six insulinomas and three of 17 endocrine pancreatic tumours. The presence of sorbin was not associated with a specific clinical syndrome.
Conclusions: Sorbin is present in the digestive tract in several forms. It is expressed in some intestinal and pancreatic endocrine tumours.
Figures






References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources