

Coil occlusion of the parent artery for treatment of symptomatic peripheral intracranial aneurysms
- PMID: 10669239
- PMCID: PMC7976354
Coil occlusion of the parent artery for treatment of symptomatic peripheral intracranial aneurysms
Abstract
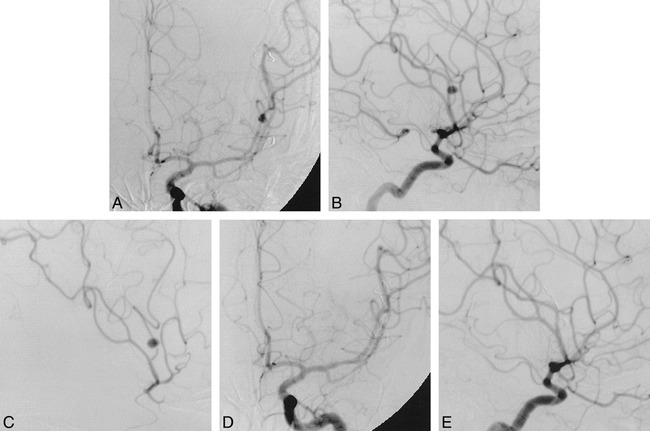
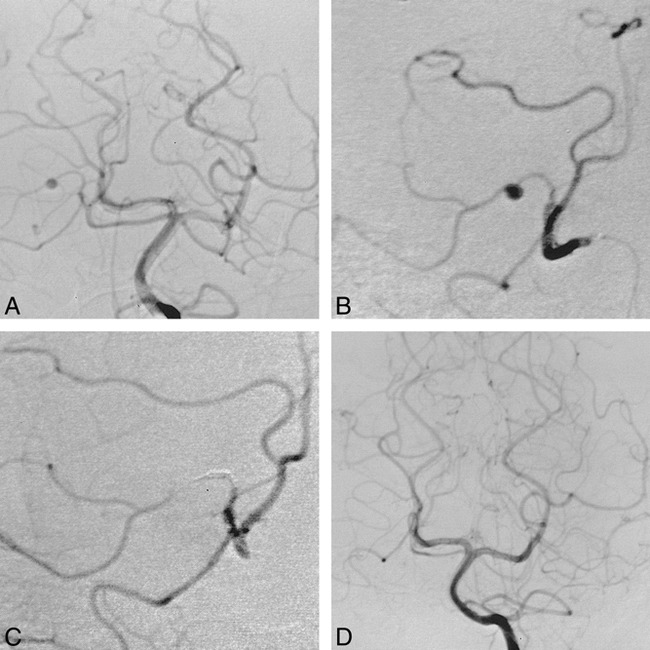
Background and purpose: Peripheral intracranial aneurysms can be difficult to treat with traditional surgical or embolization techniques that spare the parent vessel. We report the results of our use of coil occlusion of the parent vessel for the treatment of nine peripheral intracranial aneurysms.
Methods: During approximately a 4-year period, nine patients (six men and three women, 27 to 68 years old; average age, 42 years) presented to our institution with peripheral intracranial aneurysms. The aneurysms were located on branches of the right posterior inferior cerebellar artery (n = 2), the right superior cerebellar artery (n = 1), the right anterior inferior cerebellar artery (n = 1), the right posterior cerebral artery (n = 3), the left middle cerebral artery (n = 1), and the left anterior cerebral artery (n = 1). Parent vessel occlusion was performed using microcoils after test injection with amobarbital (Amytal) in eight of the nine cases (one patient was comatose and could not be tested before occlusion).
Results: Angiography immediately after the procedure showed aneurysmal occlusion in every patient. Follow-up arteriography, performed in six patients 2 to 12 months after treatment, documented continued aneurysmal occlusion in every case. Three patients exhibited mild, nondisabling neurologic deficits after coil placement; the rest had no new deficits, although one patient was severely disabled from the initial hemorrhage and one patient died of an unrelated cause.
Conclusion: Our results lend support to the use of parent vessel occlusion for peripheral aneurysms that are difficult to treat surgically or that are not amenable to intra-aneurysmal coil placement.
Figures
References
-
- Martin D, Rodesch G, Alvarez H, Lasjaunias P. Preliminary results of embolization of nonsurgical intracranial aneurysms with GD coils: the 1st year of their use. Neuroradiology 1996;38:S142-S150 - PubMed
-
- Hunt WE, Hess RM. Surgical risk as related to time of intervention in the repair of intracranial aneurysms. J Neurosurg 1968;28:14-20 - PubMed
-
- Stehbens WE. Etiology of I.C. berry aneurysms. J Neurosurg 1989;70:823-831 - PubMed
-
- Berenstein A, Ransohoff J, Kupersmith M, Flamm E, Graeb D. Transvascular treatment of giant aneurysms of the cavernous carotid and vertebral arteries. Surg Neurol 1984;21:3-12 - PubMed
-
- Fox AJ, Vinuela F, Pelz DM, et al. Use of detachable balloons for proximal artery occlusion in the treatment of unclippable cerebral aneurysms. J Neurosurg 1987;66:40-46 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical