

Case Reports
Idiopathic sclerotic inflammation of the orbit with left optic nerve compression in a patient with multifocal fibrosclerosis
Affiliations
- PMID: 10669249
- PMCID: PMC7976342
Item in Clipboard
Case Reports
Idiopathic sclerotic inflammation of the orbit with left optic nerve compression in a patient with multifocal fibrosclerosis
AJNR Am J Neuroradiol.
2000 Jan.
Abstract
We present the MR imaging findings in a 43-year-old male patient with bilateral idiopathic sclerosing inflammation of the orbit. Bilateral enhancing retrobulbar masses, with concentric compression of the retrobulbar segment of the left optic nerve, were seen. MR imaging proved to be the only means to distinguish between the different intraorbital structures and to determine the exact site of optic nerve compression. To our knowledge, this is the first documented case of MR imaging findings of this entity.
Figures
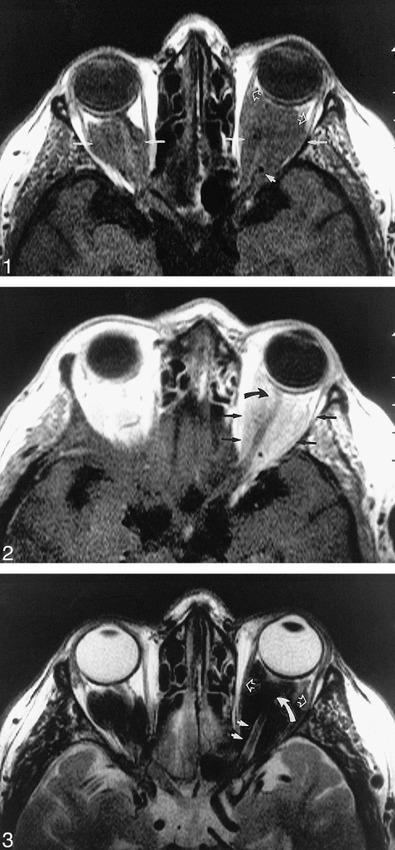
Axial unenhanced T1-weighted scan (507/15/4) [TR/TE/excitations] of the anterior skull base. Extensive homogeneous, bilateral, intraconal masses with low signal intensity are visible. The conal muscles are displaced laterally (white open arrow). The ophthalmic artery is apparent at the apex of the orbit (small white arrow).fig 2. Axial enhanced T1-weighted scan (507/15/4) of the anterior skull base. Marked homogeneous enhancement of the intraconal masses (black arrow) is visible. The left optic nerve is encircled and compressed by the retrobulbar enhancing masses and appears thinned at its distal segment (curved black arrow). There is no pathologic enhancement of the intracranial structures.fig 3. Axial turbo spin-echo T2-weighted image (2000/120/6) of the anterior skull base. Bilateral, marked hypointense, intraconal, retrobulbar masses are visible. The laterally displaced conal muscles (white open arrows) and the posterior segment of the left optic nerve and its subarachnoid space (small white arrows) are clearly apparent. The more distal segment of the subarachnoid space of the left optic nerve is compressed (curved white arrow)
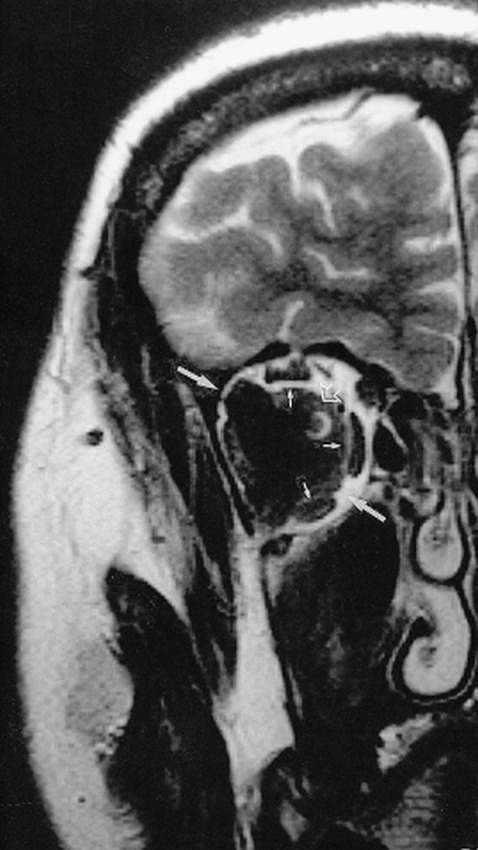
Coronal turbo spin-echo T2-weighted image (2027/120/6) of the anterior skull base. An expanding retrobulbar mass with low signal intensity is visible in the right orbit (white arrow). The conal muscles are displaced without signs of infiltration (small white arrows). In the medial and upper quadrant of this mass, the optic nerve and its subarachnoid space are clearly visible (open white arrow)
Similar articles
-
Documented optic disc cupping in compressive optic neuropathy.Ophthalmology. 1995 Nov;102(11):1577-8. doi: 10.1016/s0161-6420(13)31810-7. Ophthalmology. 1995. PMID: 9098243 No abstract available.
-
Orbital hydatid cyst: CT and MRI.Neuroradiology. 1997 Jul;39(7):512-5. doi: 10.1007/s002340050456. Neuroradiology. 1997. PMID: 9258930
-
Erdheim-Chester disease: MR imaging, anatomic, and histopathologic correlation of orbital involvement.AJNR Am J Neuroradiol. 2004 Apr;25(4):627-30. AJNR Am J Neuroradiol. 2004. PMID: 15090356 Free PMC article.
-
Anterior temporal chordoid meningioma causing compressive optic neuropathy.Optom Vis Sci. 2011 May;88(5):645-51. doi: 10.1097/OPX.0b013e3182114320. Optom Vis Sci. 2011. PMID: 21358445 Review.
-
Orbital disease, optic nerve and chiasm.Curr Opin Neurol. 1997 Feb;10(1):22-30. doi: 10.1097/00019052-199702000-00006. Curr Opin Neurol. 1997. PMID: 9099523 Review.
Cited by
-
Clinical presentation and organ-based outcomes of Multifocal fibrosclerosis: A systematic review.SAGE Open Med. 2023 May 29;11:20503121231178046. doi: 10.1177/20503121231178046. eCollection 2023. SAGE Open Med. 2023. PMID: 37275844 Free PMC article. Review.
References
-
- Rootman J, McCarthy M, White V, Harris G, Kennerdell , Idiopathic sclerosing inflammation of the orbit. A distinct clinicopathologic entity. Ophthalmology 1994;101:570-584 - PubMed
-
- Comings DE, Skubi KB, VanEyes J, Motulsky AG. Familial multifocal fibrosclerosis. Ann Intern Med 1967;66:884-892 - PubMed
-
- Richards AB, Skalka HW, Roberts FJ, Flint A. Pseudotumour of the orbit and retroperitoneal fibrosis. Arch Ophthalmol 1980;98:1617-1620 - PubMed
-
- Früh D, Jaeger W, Käfer O, Orbital involvement in retroperitoneal fibrosis (morbus Ormond). Mod Probl Ophthalmol 1975;14:651-656 - PubMed
-
- Friberg TR, Steward T. Ocular involvement in systemic idiopathic fibrosis. Retina 1983;3:34-39
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical