

Cost-effectiveness of low-molecular-weight heparin in the treatment of proximal deep vein thrombosis
- PMID: 10672114
- PMCID: PMC1495337
- DOI: 10.1046/j.1525-1497.2000.03349.x
Cost-effectiveness of low-molecular-weight heparin in the treatment of proximal deep vein thrombosis
Abstract
Objective: To estimate the cost-effectiveness of low-molecular-weight heparin (LMWH) in the treatment of proximal lower extremity deep venous thrombosis.
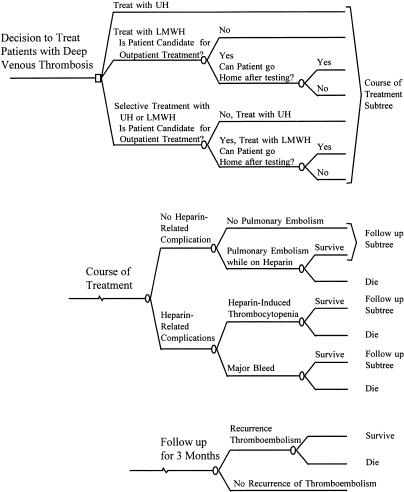
Design: Cost-effectiveness analysis that includes the treatment of the index case and simulated 3-month follow-up.
Setting: Acute care facility.
Patients and participants: Hypothetical cohorts of 1,000 patients who present with proximal deep venous thrombosis.
Interventions: Intravenous unfractionated heparin (UH), LMWH (40% at home, 60% in hospital), or selective UH/LMWH (UH for hospitalized patients and LMWH for patients treated at home).
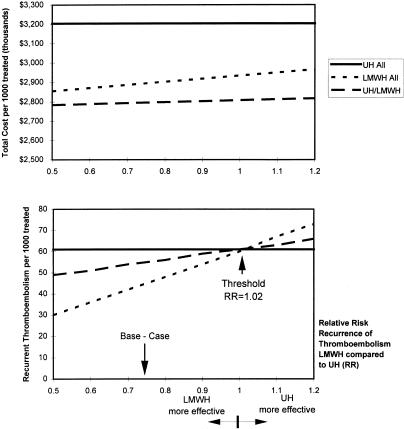
Measurements and main results: The outcomes were recurrent thrombosis, mortality, direct medical costs, and marginal cost-effectiveness ratios from the payer's perspective. At the base-case and under most assumptions in the sensitivity analysis, the LMWH and the selective UH/LMWH strategies dominate the UH strategy i.e., they result in fewer cases of recurrent thrombosis and fewer deaths, and they save resources. The savings occur primarily by decreasing the length of stay. The LMWH strategy resulted in lower costs as compared with the UH strategy when the proportion of patients treated at home was more than 14%. Treating 1, 000 patients with the LMWH strategy as compared with the UH/LMWH strategy would result in 10 fewer cases of recurrent thrombosis, 1.2 fewer deaths, at an additional cost of $96,822; the cost-effectiveness ratio was $9,667 and $80,685 per recurrent thrombosis or death prevented, respectively.
Conclusions: Treatment with LMWH leads to savings and better outcomes as compared with UH in patients with lower extremity deep venous thrombosis. The selective UH/LMWH strategy is an alternative option.
Figures
Similar articles
-
Low-molecular-weight heparins compared with unfractionated heparin for treatment of acute deep venous thrombosis. A cost-effectiveness analysis.Ann Intern Med. 1999 May 18;130(10):789-99. doi: 10.7326/0003-4819-130-10-199905180-00002. Ann Intern Med. 1999. PMID: 10366368
-
A probabilistic cost-effectiveness analysis of enoxaparin versus unfractionated heparin for the prophylaxis of deep-vein thrombosis following major trauma.Can J Clin Pharmacol. 2007 Summer;14(2):e215-26. Epub 2007 Jun 6. Can J Clin Pharmacol. 2007. PMID: 17652767
-
Cost-effectiveness of low-molecular-weight heparin and unfractionated heparin in treatment of deep vein thrombosis.CMAJ. 1998 Oct 20;159(8):931-8. CMAJ. 1998. PMID: 9834718 Free PMC article.
-
Low-molecular-weight heparin (LMWH) in the treatment of thrombosis.Eur J Med Res. 2004 Apr 30;9(4):225-39. Eur J Med Res. 2004. PMID: 15210403 Review.
-
Cost effectiveness of desirudin compared with a low molecular weight heparin in the prevention of deep vein thrombosis after total hip replacement surgery.Pharmacoeconomics. 2001;19(5 Pt 2):589-97. doi: 10.2165/00019053-200119050-00012. Pharmacoeconomics. 2001. PMID: 11465303 Review.
Cited by
-
Cost effectiveness of bemiparin sodium versus unfractionated heparin and oral anticoagulants in the acute and long-term treatment of deep vein thrombosis.Pharmacoeconomics. 2006;24(1):81-92. doi: 10.2165/00019053-200624010-00007. Pharmacoeconomics. 2006. PMID: 16445305
-
The potential benefits of low-molecular-weight heparins in cancer patients.J Hematol Oncol. 2010 Jan 14;3:3. doi: 10.1186/1756-8722-3-3. J Hematol Oncol. 2010. PMID: 20074349 Free PMC article. Review.
-
The best of JGIM.J Gen Intern Med. 2002 Dec;17(12):952-5. doi: 10.1046/j.1525-1497.2002.21012.x. J Gen Intern Med. 2002. PMID: 12472932 Free PMC article. No abstract available.
-
Blunt carotid injury.Curr Treat Options Cardiovasc Med. 2006 Apr;8(2):167-73. doi: 10.1007/s11936-006-0009-7. Curr Treat Options Cardiovasc Med. 2006. PMID: 16533491
-
Adherence to Venous Thromboprophylaxis Guidelines for Medical and Surgical Inpatients of Teaching Hospitals, Shiraz-Iran.Tanaffos. 2015;14(1):17-26. Tanaffos. 2015. PMID: 26221148 Free PMC article.
References
-
- Hirsh J, Hoak J. Management of deep vein thrombosis and pulmonary embolism: a statement for healthcare professionals. Council on Thrombosis (in consultation with the Council on Cardiovascular Radiology), American Heart Association. Circulation. 1996;93:2212–45. - PubMed
-
- Prandoni P, Lensing AW, Cogo A, et al. The long-term clinical course of acute deep venous thrombosis. Ann Intern Med. 1996;125:1–7. - PubMed
-
- Raschke RA, Reilly BM, Guidry JR, Fontana JR, Srinivas S. The weight-based heparin dosing nomogram compared with a “standard care” nomogram: a randomized controlled trial. Ann Intern Med. 1993;119:874–81. - PubMed
-
- Hirsh J, Warkentin TE, Raschke R, Granger C, Ohman EM, Dalen JE. Heparin and low-molecular-weight heparin: mechanisms of action, pharmacokinetics, dosing considerations, monitoring, efficacy, and safety. Chest. 1998;114:489S–510S. - PubMed
-
- Hyers TM. Venous thromboembolism. Am J Respir Crit Care Med. 1999;159:1–14. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical