

The epidemiology of antibiotic resistance in hospitals: paradoxes and prescriptions
- PMID: 10677558
- PMCID: PMC26540
- DOI: 10.1073/pnas.97.4.1938
The epidemiology of antibiotic resistance in hospitals: paradoxes and prescriptions
Abstract
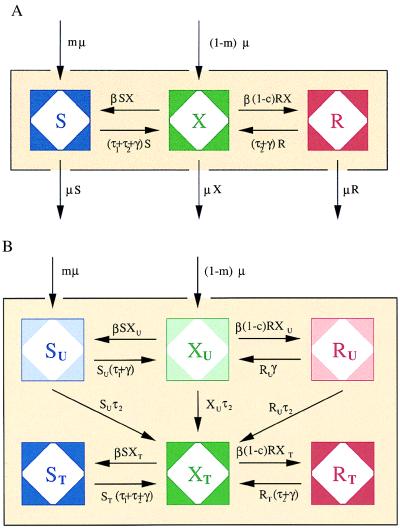
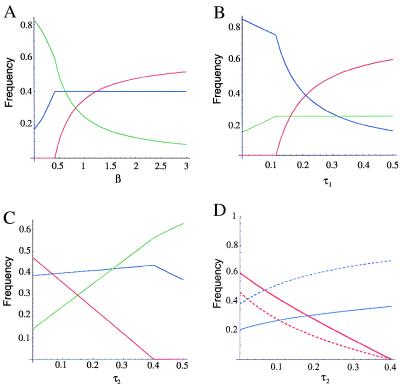
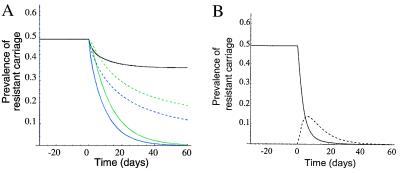
A simple mathematical model of bacterial transmission within a hospital was used to study the effects of measures to control nosocomial transmission of bacteria and reduce antimicrobial resistance in nosocomial pathogens. The model predicts that: (i) Use of an antibiotic for which resistance is not yet present in a hospital will be positively associated at the individual level (odds ratio) with carriage of bacteria resistant to other antibiotics, but negatively associated at the population level (prevalence). Thus inferences from individual risk factors can yield misleading conclusions about the effect of antibiotic use on resistance to another antibiotic. (ii) Nonspecific interventions that reduce transmission of all bacteria within a hospital will disproportionately reduce the prevalence of colonization with resistant bacteria. (iii) Changes in the prevalence of resistance after a successful intervention will occur on a time scale of weeks to months, considerably faster than in community-acquired infections. Moreover, resistance can decline rapidly in a hospital even if it does not carry a fitness cost. The predictions of the model are compared with those of other models and published data. The implications for resistance control and study design are discussed, along with the limitations and assumptions of the model.
Figures
References
-
- Gaynes R, Monnet D. Ciba Found Symp. 1997;207:47–56. ; discussion 56–60. - PubMed
-
- Monnet D L, Archibald L K, Phillips L, Tenover F C, McGowan J E, Jr, Gaynes R P. Infect Control Hosp Epidemiol. 1998;19:388–394. - PubMed
-
- Bonten M J, Weinstein R A. Infect Control Hosp Epidemiol. 1996;17:193–200. - PubMed
-
- Gaynes R P, Weinstein R A, Smith J, Carman M, Kabins S A. Infect Control. 1983;4:221–224. - PubMed
-
- Slaughter S, Hayden M K, Nathan C, Hu T C, Rice T, Van Voorhis J, Matushek M, Franklin C, Weinstein R A. Ann Intern Med. 1996;125:448–456. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
