

Testosterone replacement and resistance exercise in HIV-infected men with weight loss and low testosterone levels
- PMID: 10683055
- PMCID: PMC3173037
- DOI: 10.1001/jama.283.6.763
Testosterone replacement and resistance exercise in HIV-infected men with weight loss and low testosterone levels
Abstract
Context: Previous studies of testosterone supplementation in HIV-infected men failed to demonstrate improvement in muscle strength. The effects of resistance exercise combined with testosterone supplementation in HIV-infected men are unknown.
Objective: To determine the effects of testosterone replacement with and without resistance exercise on muscle strength and body composition in HIV-infected men with low testosterone levels and weight loss.
Design and setting: Placebo-controlled, double-blind, randomized clinical trial conducted from September 1995 to July 1998 at a general clinical research center.
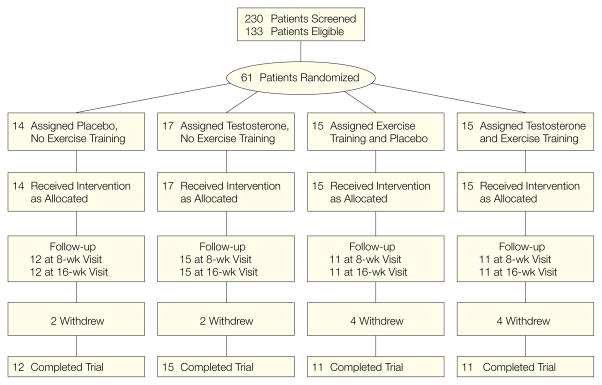
Participants: Sixty-one HIV-infected men aged 18 to 50 years with serum testosterone levels of less than 12.1 nmol/L (349 ng/dL) and weight loss of 5% or more in the previous 6 months, 49 of whom completed the study.
Interventions: Participants were randomly assigned to 1 of 4 groups: placebo, no exercise (n = 14); testosterone enanthate (100 mg/wk intramuscularly), no exercise (n = 17); placebo and exercise (n = 15); or testosterone and exercise (n = 15). Treatment duration was 16 weeks.
Main outcome measures: Changes in muscle strength, body weight, thigh muscle volume, and lean body mass compared among the 4 treatment groups.
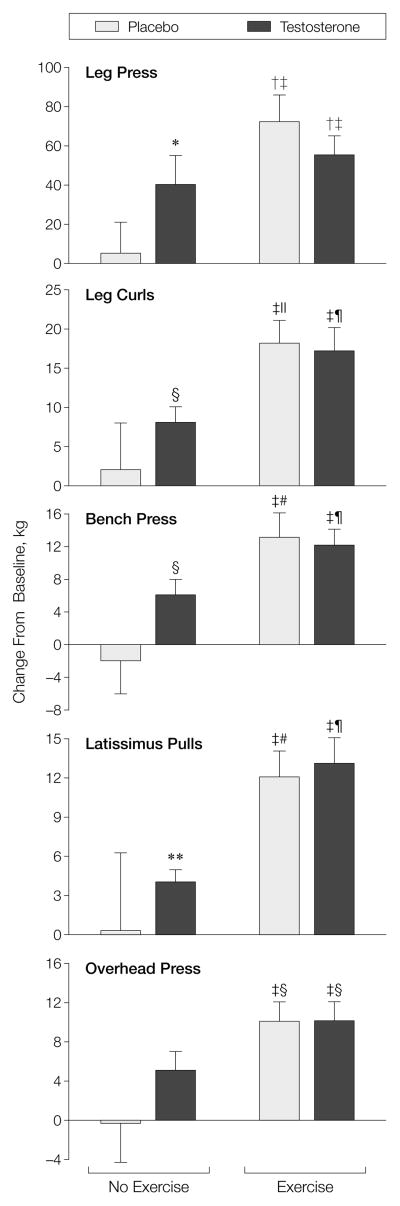
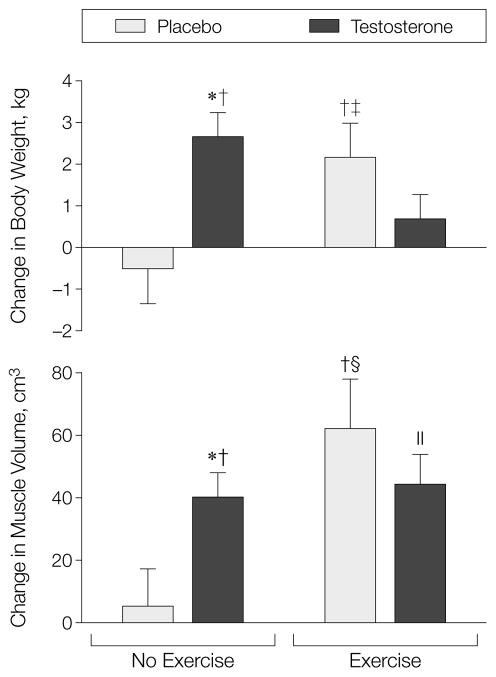
Results: Body weight increased significantly by 2.6 kg (P<.001) in men receiving testosterone alone and by 2.2 kg (P = .02) in men who exercised alone but did not change in men receiving placebo alone (-0.5 kg; P = .55) or testosterone and exercise (0.7 kg; P = .08). Men treated with testosterone alone, exercise alone, or both experienced significant increases in maximum voluntary muscle strength in leg press (range, 22%-30%), leg curls (range, 18%-36%), bench press (range, 19%-33%), and latissimus pulls (range, 17%-33%). Gains in strength in all exercise categories were greater in men assigned to the testosterone-exercise group or to the exercise-alone group than in those assigned to the placebo-alone group. There was a greater increase in thigh muscle volume in men receiving testosterone alone (mean change, 40 cm3; P<.001 vs zero change) or exercise alone (62 cm3; P = .003) than in men receiving placebo alone (5 cm3; P = .70). Average lean body mass increased by 2.3 kg (P = .004) and 2.6 kg (P<.001), respectively, in men who received testosterone alone or testosterone and exercise but did not change in men receiving placebo alone (0.9 kg; P = .21). Hemoglobin levels increased in men receiving testosterone but not in those receiving placebo.
Conclusion: Our data suggest that testosterone and resistance exercise promote gains in body weight, muscle mass, muscle strength, and lean body mass in HIV-infected men with weight loss and low testosterone levels. Testosterone and exercise together did not produce greater gains than either intervention alone.
Figures
Comment in
-
Exercise regimens for men with HIV.JAMA. 2000 Jul 12;284(2):175-6. doi: 10.1001/jama.284.2.175. JAMA. 2000. PMID: 10889580 No abstract available.
References
-
- Kotler DP, Tierney AR, Ferraro R, Francisco A, Wang J, Pierson RN., Jr The magnitude of body cell mass depletion determines the timing of death from wasting in AIDS. Am J Clin Nutr. 1989;50:444–447. - PubMed
-
- Chlebowski RT, Grosvenor MB, Bernhard NH, Morales LS, Bulcavage LM. Nutritional status, gastrointestinal dysfunction and survival in patients with AIDS. Am J Gastroenterol. 1989;84:1288–1293. - PubMed
-
- Linden CP, Allen S, Serufilira A, et al. Predictors of mortality among HIV-infected women in Kigali, Rwanda. Ann Intern Med. 1992;116:320–328. - PubMed
-
- Sellmeyer DE, Grunfeld C. 1996 Endocrine and metabolic disturbances in human immunodeficiency virus infection and the acquired immune deficiency syndrome. Endocr Rev. 1996;17:518–52. - PubMed
-
- Dobs AS, Dempsey MA, Landeson PW, Polk BF. Endocrine disorders in men infected with human immunodeficiency virus. Am J Med. 1988;84:611–615. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
