

Short-term arteriographic and clinical outcome after cerebral angioplasty and stenting for intracranial vertebrobasilar and carotid atherosclerotic occlusive disease
- PMID: 10696004
- PMCID: PMC7975354
Short-term arteriographic and clinical outcome after cerebral angioplasty and stenting for intracranial vertebrobasilar and carotid atherosclerotic occlusive disease
Abstract
Background and purpose: The safe performance of percutaneous transluminal cerebral angioplasty for intracranial atherosclerotic lesions requires that the risk of complications, such as acute occlusion or symptomatic dissection, and restenosis be reduced. Our purpose was to assess the effectiveness, safety, and short-term arteriographic and clinical outcome of cerebral angioplasty and stenting (CAS) for intracranial vertebrobasilar and distal internal carotid atherosclerotic occlusive lesions.
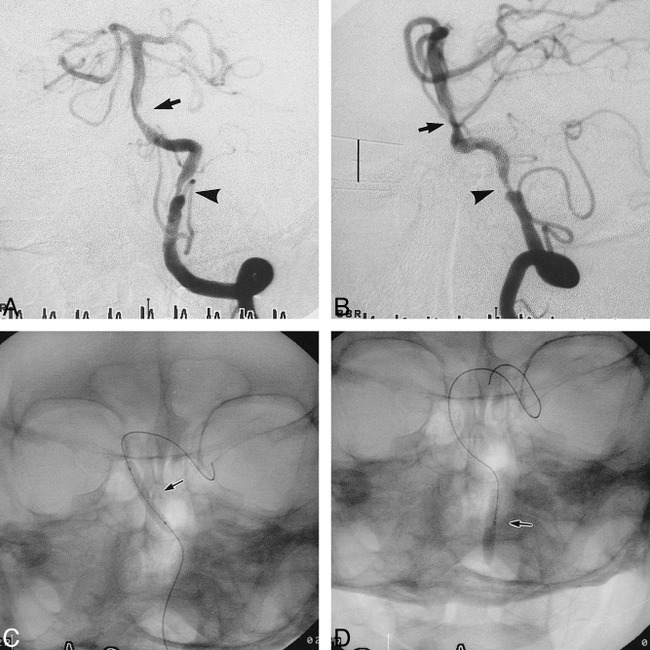
Methods: Between March 1998 and November 1998, 10 patients with 12 intracranial atherosclerotic lesions of the vertebrobasilar artery and the distal internal carotid artery underwent treatment with flexible balloon-expandable coronary stents.
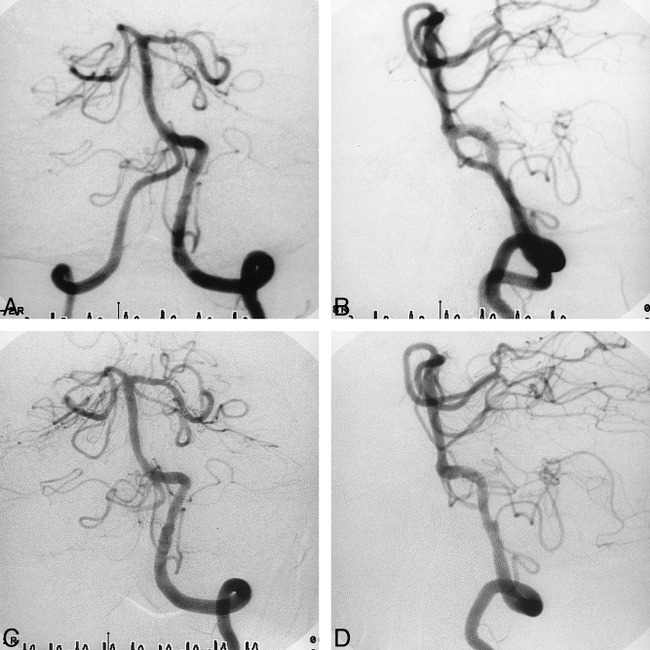
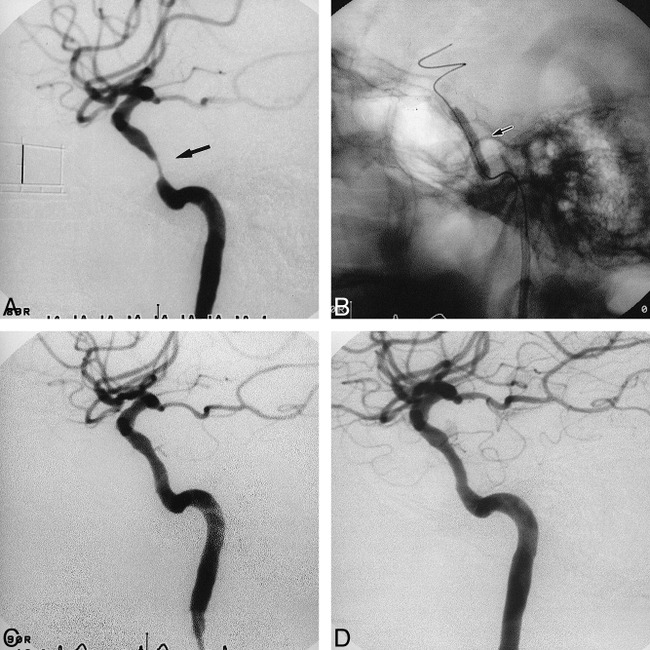
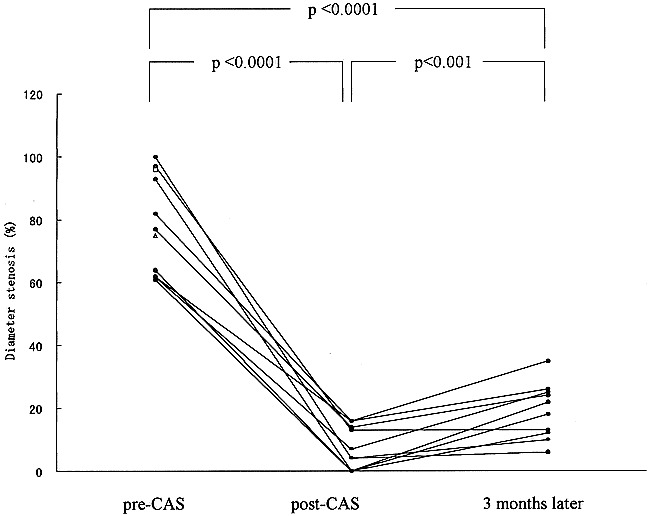
Results: Although in two of the 10 patients CAS was not successful because of the inability to access the site of arterial stenosis, 10 lesions in eight patients were successfully dilated with stents. No complications occurred during or after the procedure and no neurologic ischemic events or restenoses occurred during the follow-up period.
Conclusion: CAS appears to be a safe and effective means for treating intracranial atherosclerotic occlusive disease, yielding a favorable arteriographic and clinical outcome.
Figures
References
-
- Sundt TM Jr, Smith HC, Campbell JK, Vlietstra RE, Cucchiara RF, Stanson AW. Transluminal angioplasty for basilar artery stenosis. Mayo Clin Proc 1980;55:673-680 - PubMed
-
- Clark WM, Barnwell SL, Nesbit G, O'Neil OR, Wynn ML, Coull BM. Safety and efficacy of percutaneous transluminal angioplasty for intracranial atherosclerotic stenosis. Stroke 1995;26:1200-1204 - PubMed
-
- Honda S, Mori T, Fukuoka M, et al. Successful percutaneous transluminal angioplasty of the intracranial vertebral artery 1 month after total occlusion. Neurol Med Chir (Tokyo) 1994;34:551-554 - PubMed
-
- Mori T, Mori K, Fukuoka M, Honda S. Percutaneous transluminal cerebral angioplasty for total occlusion of middle cerebral arteries. Neuroradiology 1997;39:71-74 - PubMed
-
- Higashida RT, Tsai FY, Halbach VV, Dowd CF, Hieshima GB. Cerebral percutaneous transluminal angioplasty. Heart Dis Stroke 1993;2:497-502 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources