

The retrograde approach: a consideration for the endovascular treatment of aneurysms
- PMID: 10696006
- PMCID: PMC7975343
The retrograde approach: a consideration for the endovascular treatment of aneurysms
Abstract
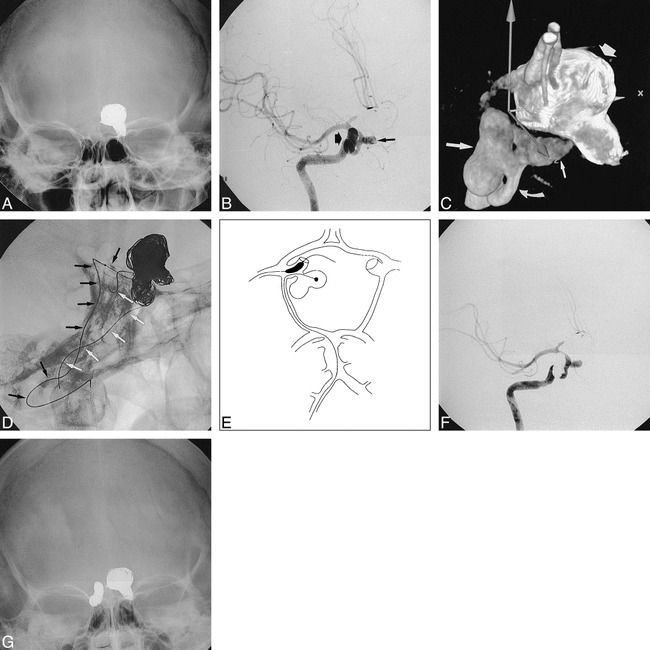
Background and purpose: The traditional endovascular approach to a cerebral aneurysm is anterograde, with the embolization and balloon protection catheters introduced via the parent vessel. Unfortunately, this approach may be restrictive, because these catheters cannot always be navigated at an optimal angle into the arterial branch that needs balloon protection or the part of the aneurysm that needs coiling. The purpose of this study was to determine the efficacy of a retrograde approach.
Methods: Twelve patients, seven women and five men, 28 to 65 years old (mean age, 45 years), were treated via the retrograde approach between March 1998 and February 1999. Three patients were treated for acutely ruptured aneurysms following subarachnoid hemorrhage. The rest had asymptomatic, unruptured aneurysms.
Results: We were able to accomplish endovascular treatment in 10 cases. In the other two, the attempted retrograde route of access could not be achieved. The treatment afforded complete embolization in nine of the 10 patients. Symptomatic distal clot embolization occurred in one patient who had some residual, albeit improving, deficits at discharge. No other patients worsened with the treatment. There were two intraprocedural aneurysmal ruptures. None of the aneurysms restudied within 6 months (eight of 12) showed evidence of recanalization.
Conclusion: Our results indicate that it is possible to safely and effectively access a cerebral aneurysm via a retrograde approach. We believe that the anatomic benefits afforded by this technique outweigh the potential risks associated with the catheterization of another major cerebral arterial feeder.
Figures

References
-
- Viñuela F, Duckwiler G, Mawad M. Guglielmi detachable coil embolization of acute intracranial aneurysm: perioperative anatomical and clinical outcome in 403 patients. J Neurosurg 1997;86:475-482 - PubMed
-
- Moret J, Cognard C, Weill A, Castings L, Rey A. The “remodeling technique” in the treatment of wide neck intracranial aneurysms: angiographic results and clinical follow-up in 56 cases. Interv Neuroradiol 1997;3:21-35 - PubMed
-
- Higashida RT, Smith W, Gress D, et al. Intravascular stent and endovascular coil placement for a ruptured fusiform aneurysm of the basilar artery. J Neurosurg 1997;87:944-949 - PubMed
-
- Lylyk P, Ceratto R, Hurvitz D, Basso A. Treatment of a vertebral dissecting aneurysm with stents and coils: technical case report. Neurosurgery 1998;43:385-388 - PubMed
-
- Mericle RA, Lanzino G, Wakhloo AK, Guterman LR, Hopkins LN. Stenting and secondary coiling of intracranial internal carotid artery aneurysm: technical case report. Neurosurgery 1998;43:1229-1234 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical