

Comparison of relative cerebral blood volume and proton spectroscopy in patients with treated gliomas
- PMID: 10696024
- PMCID: PMC7975338
Comparison of relative cerebral blood volume and proton spectroscopy in patients with treated gliomas
Abstract
Background and purpose: Elevated relative regional cerebral blood volume (rCBV) reflects the increased microvascularity that is associated with brain tumors. The purpose of this study was to investigate the potential role of rCBV in the determination of recurrent/residual disease in patients with treated gliomas.
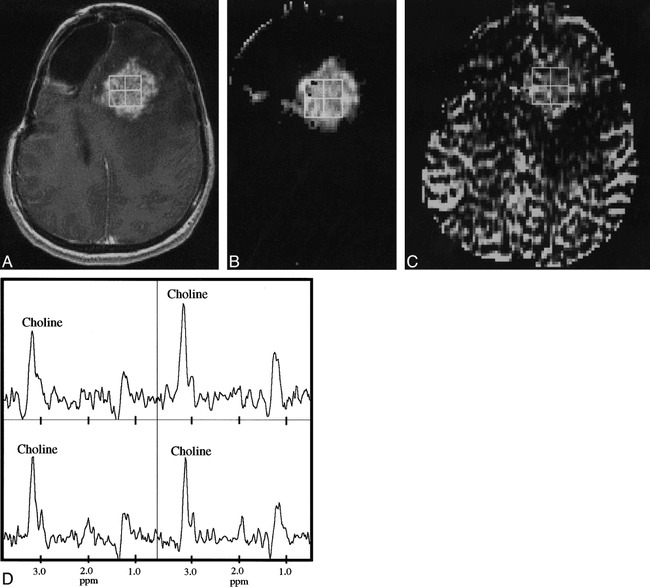
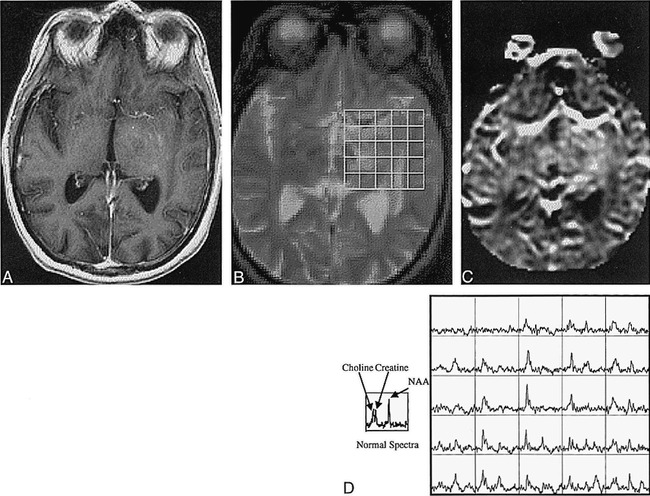
Methods: Thirty-one rCBV studies were performed in 19 patients with treated gliomas. All patients also had proton MR spectroscopy and conventional MR imaging. Regions of abnormality were identified on conventional MR images by two neuroradiologists and compared with rCBV and MR spectroscopic data. Metabolites and rCBV were quantified and compared in abnormal regions.
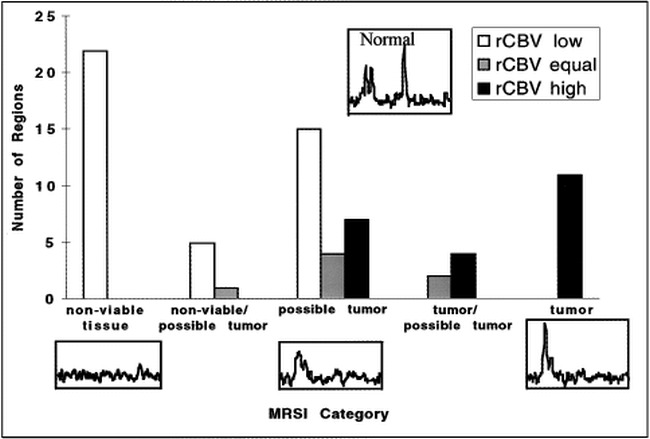
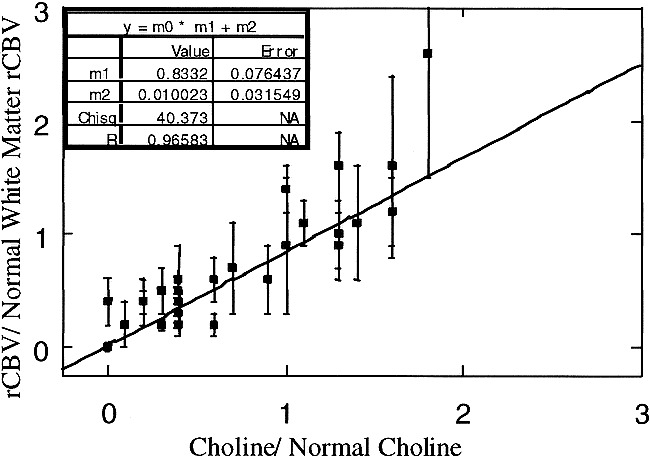
Results: In high-grade tumors, rCBV values were proportional to choline in regions of tumor and nonviable tissue. Although the presence of residual/recurrent disease was often ambiguous on conventional MR images, the rCBV maps indicated regions of elevated vascularity in all low-grade tumors and in 12 of 17 grade IV lesions. Regions of elevated and low rCBV corresponded well with spectra, indicating tumor and nonviable tissue, respectively.
Conclusion: This study suggests that rCBV maps and MR spectroscopy are complementary techniques that may improve the detection of residual/recurrent tumor in patients with treated gliomas. Compared with the spectra, the rCBV maps may better reflect the heterogeneity of the tumor regions because of their higher resolution. The multiple markers of MR spectroscopy enable better discrimination between normal and abnormal tissue than do the rCBV maps.
Figures
References
-
- Aronen HJ, Cohen MS, Belliveau JW, Fordham JA, Rosen BR. Ultrafast imaging of brain tumors. Top Magn Reson Imaging 1993;5:14-24 - PubMed
-
- Rosen BR, Belliveau JW, Chien D. Perfusion imaging by nuclear magnetic resonance. Magn Reson Q 1989;5:263-281 - PubMed
-
- Maeda M, Itoh S, Kimura H, et al. Tumor vascularity in the brain: evaluation with dynamic susceptibility-contrast MR imaging. Radiology 1993;189:233-238 - PubMed
-
- Guckel F, Brix G, Rempp K, Deimling M, Rother J, Georgi M. Assessment of cerebral blood volume with dynamic susceptibility contrast enhanced gradient-echo imaging. J Comput Assist Tomogr 1994;18:344-351 - PubMed
-
- Aronen HJ, Gazit IE, Louis DN, et al. Cerebral blood volume maps of gliomas: comparison with tumor grade and histologic findings. Radiology 1994;191:41-51 - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical