

Outcome of pancreaticoduodenectomy with pylorus preservation or with antrectomy in the treatment of chronic pancreatitis
- PMID: 10714621
- PMCID: PMC1420999
- DOI: 10.1097/00000658-200003000-00001
Outcome of pancreaticoduodenectomy with pylorus preservation or with antrectomy in the treatment of chronic pancreatitis
Abstract
Objective: To compare the short- and long-term results of pancreaticoduodenectomy with pylorus preservation (PPPD) or with antrectomy (Whipple procedure) in the treatment of selected patients with chronic pancreatitis.
Background: PPPD may be preferred over Whipple because of its purported nutritional advantages and the reduced likelihood of postgastrectomy syndromes.
Methods: A retrospective review was performed of 72 consecutive patients undergoing pancreaticoduodenectomy for chronic pancreatitis between 1991 and 1997.
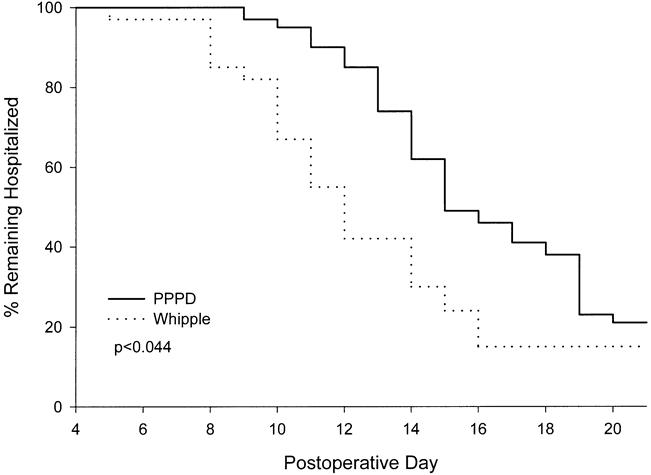
Results: PPPD was performed in 39 patients and Whipple in 33. The two patient populations had similar characteristics. Short-term complications included (PPPD vs. Whipple): pancreatic or biliary fistulas (5.1% vs. 15%), delayed gastric emptying (33% vs. 12%), cholangitis (2.6% vs. 6.1%), and death (0 vs. 3%). Delayed gastric emptying was not associated with other complications and resulted in longer hospital stays for PPPD than for Whipple patients (15 vs. 12 days). The duration of follow-up averaged 41 +/- 24 months. Long-term weight status was similar, with body-mass indices of 22.1 and 22.9 after PPPD and Whipple, respectively. Postoperative enzyme supplementation (63% vs. 77%) and new-onset diabetes (10% vs. 12%) did not differ significantly between the PPPD and Whipple groups. Dumping, bile gastritis, or peptic ulcer disease occurred in three patients after PPPD and in three after Whipple. Complete or partial pain relief was attained in 60% and 70% of patients after PPPD and Whipple, respectively. Multivariate analysis of preoperative variables revealed that site-specific pathology in the head of the pancreas was the only independent factor associated with successful pain relief after pancreatic resection.
Conclusion: PPPD results in higher frequencies of postoperative delayed gastric emptying compared with the Whipple procedure. Both operations achieve comparable long-term nutritional results, cause new insulin dependence in surprisingly few patients, and provide equivalent pain relief to 65% of selected patients. Patients with disproportionate pathology in the head of the pancreas have a higher likelihood of successful pain relief.
Figures
Comment in
-
Whipple or pylorus preservation? A critical reappraisal and some new insights into pancreaticoduodenectomy.Ann Surg. 2000 Mar;231(3):301-2. doi: 10.1097/00000658-200003000-00002. Ann Surg. 2000. PMID: 10714622 Free PMC article. No abstract available.
References
-
- Warshaw AL, Banks PA, Fernandez-del Castillo C. AGA technical review: treatment of pain in chronic pancreatitis. Gastroenterology 1998; 115:765–776. - PubMed
-
- Warshaw AL. Conservation of pancreatic tissue by combined gastric, biliary, and pancreatic duct drainage for pain from chronic pancreatitis. Am J Surg 1985; 149:563–569. - PubMed
-
- Jalleh RP, Aslam M, Williamson RC. Pancreatic tissue and ductal pressures in chronic pancreatitis. Br J Surg 1991; 78:1235–1237. - PubMed
-
- Prinz RA, Greenlee HB. Pancreatic duct drainage in chronic pancreatitis. Hepatogastroenterology 1990; 37:295–300. - PubMed
-
- Holmberg JT, Isaksson G, Ihse I. Long-term results of pancreaticojejunostomy in chronic pancreatitis. Surg Gynecol Obstet 1985; 160:339–346. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
