

Local excision of rectal cancer without adjuvant therapy: a word of caution
- PMID: 10714627
- PMCID: PMC1421005
- DOI: 10.1097/00000658-200003000-00007
Local excision of rectal cancer without adjuvant therapy: a word of caution
Abstract
Objective: To evaluate the results of local excision alone for the treatment of rectal cancer, applying strict selection criteria.
Background data: Several retrospective studies have demonstrated that tumor control in properly selected patients with rectal cancer treated locally is comparable to that observed after radical surgery. Although there is a consensus regarding the need for patient selection for local excision, the specific criteria vary among centers.
Methods: The authors reviewed 82 patients with T1 (n = 55) and T2 (n = 27) rectal cancer treated with transanal excision only during a 10-year period. At pathologic examination, all tumors were localized to the rectal wall, had negative excision margins, were well or moderately differentiated, and had no blood or lymphatic vessel invasion, nor a mucinous component. End points were local and distant tumor recurrence and patient survival.
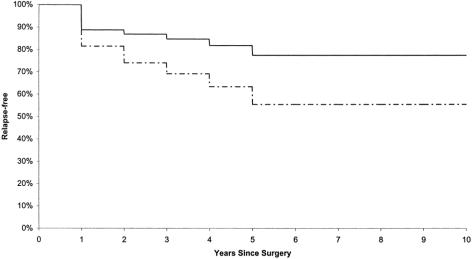
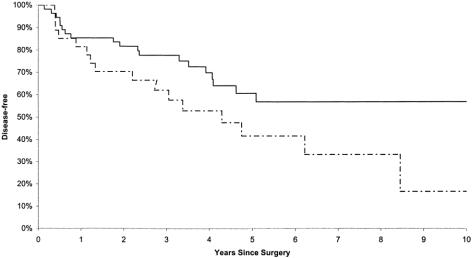
Results: Ten of the 55 patients with T1 tumors (18%) and 10 of the 27 patients with T2 tumors (37%) had recurrence at 54 months of follow-up. Average time to recurrence was 18 months in both groups. Seventeen of the 20 patients with local recurrence underwent salvage surgery. The survival rate was 98% for patients with T1 tumors and 89% for patients with T2 tumors. Preoperative staging by endorectal ultrasound did not influence local recurrence or tumor-specific survival.
Conclusion: Local excision of early rectal cancer, even in the ideal candidate, is followed by a much higher recurrence rate than previously reported. Although most patients in whom local recurrence develops can be salvaged by radical resection, the long-term outcome remains unknown.
Figures
References
-
- MacFarlane JK, Ryall RDH, Heald RJ. Mesorectal excision for rectal cancer. Lancet 1993; 341:457–460. - PubMed
-
- Enker WE, Havenga K, Polyak T, Thaler H, Cranor M. Abdominoperineal resection via total mesorectal excision and autonomic nerve preservation for low rectal cancer. World J Surg 1997; 21:715–720. - PubMed
-
- Biggers OR, Beart RW, Ilstrup DW. Local excision of rectal cancer. Dis Colon Rectum 1986; 29:374–377. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
