

Simultaneous pancreas-kidney transplantation and living related donor renal transplantation in patients with diabetes: is there a difference in survival?
- PMID: 10714635
- PMCID: PMC1421013
- DOI: 10.1097/00000658-200003000-00015
Simultaneous pancreas-kidney transplantation and living related donor renal transplantation in patients with diabetes: is there a difference in survival?
Abstract
Objective: To compare the outcome of simultaneous pancreas-kidney transplantation (SPK) and living related donor renal transplantation (LRD) in patients with diabetes.
Summary background data: It remains unanswered whether diabetic patients with end-stage renal failure are better served by LRD or SPK.
Methods: Using a longitudinal database, data from all diabetic patients receiving LRD or cadaveric renal transplants or SPKs from January 1986 through January 1996 were analyzed. Patient and graft survival, early graft function, and the cause of patient and graft loss were compared for 43 HLA-identical LRDs, 87 haplotype-identical LRDs, 379 SPKs, and 296 cadaveric renal transplants.
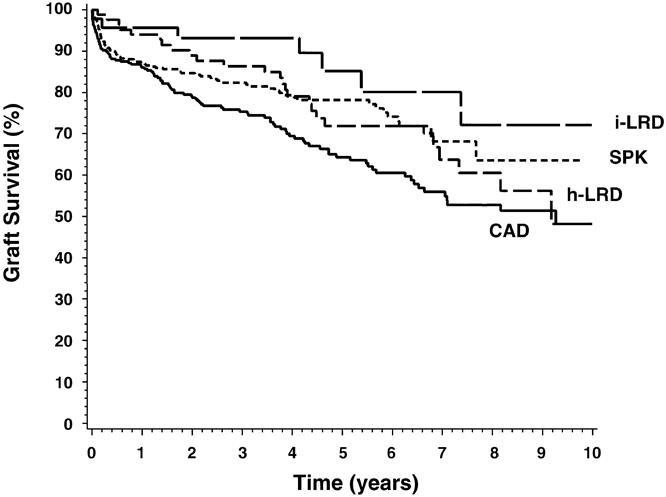
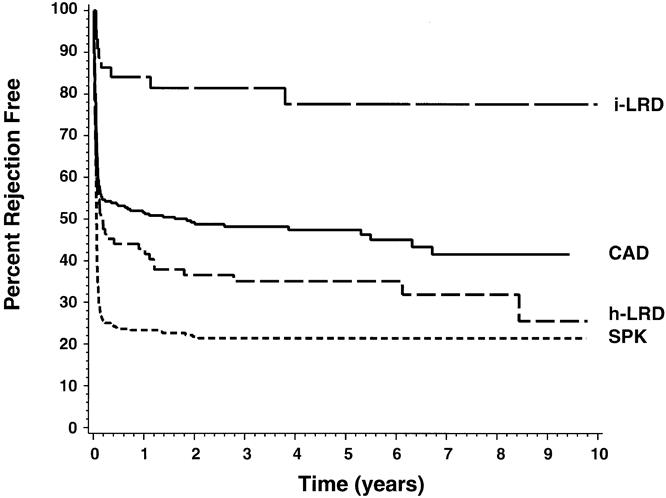
Results: The demographic composition of the SPK and LRD groups were similar, but because of less strict selection criteria in the cadaveric transplant group, patients were 10 years older, more patients received dialysis, and patients had been receiving dialysis longer before transplantation. Patient survival was similar for the SPK and LRD groups but was significantly lower for the cadaveric renal transplant group. Similarly, there was no difference in graft survival between SPK and LRD recipients, but it was significantly lower for recipients in the cadaveric renal transplant group. Delayed graft function was significantly more common in the cadaveric renal transplant group. Discharge creatinine, the strongest predictor of patient and graft survival, was highest in the SPK group and lowest in the HLA-identical LRD group. The rate of rejection within the first year was greatest in SPK patients (77%), intermediate in the haplotype-identical LRD and cadaveric transplant groups (57% and 48%, respectively), and lowest (16%) in the HLA-identical LRD group. Cardiovascular disease was the primary cause of death for all groups. Acute rejection, chronic rejection, and death with a functioning graft were the predominant causes of graft loss.
Conclusions: This study demonstrates that there was no difference in patient or graft survival in diabetic patients receiving LRD or SPK transplants. However, graft and patient survival rates in diabetic recipients of cadaveric renal transplants were significantly lower than in the other groups.
Figures

References
-
- Gruessner A, Sutherland DER. Pancreas transplantation in the United States and non-US as reported to the United Network for Organ Sharing (UNOS) and the International Pancreas Transplant Registry (IPTR). In: Cecka JM, Terasaki PI, eds. Clinical Transplants 1996. Los Angeles: UCLA Tissue Typing Laboratory; 1997: 47–67. - PubMed
-
- USRDS 1998 Annual Data Report. Reference tables E 50, 58, 66, 74, 82, 90. USRDS, April 1998.
-
- Cecka JM. The UNOS Scientific Renal Transplant Registry. In: Cecka MJ, Terasaki PI, eds. Clinical Transplants 1996. Los Angeles: UCLA Tissue Typing Laboratory; 1997: 1–14. - PubMed
-
- The Diabetes Control and Complications Trial Research Group. The effect of intensive treatment of diabetes on the development and progression of long-term complications in insulin-dependent diabetes mellitus. N Engl J Med 1993; 329:977–986. - PubMed
-
- Rosen CB, Frohnert PP, Velosa JA, Engen DE, Sterioff S. Morbidity of pancreas transplantation during cadaveric renal transplantation. Transplantation 1991; 51:123–127. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
