

Error, stress, and teamwork in medicine and aviation: cross sectional surveys
- PMID: 10720356
- PMCID: PMC27316
- DOI: 10.1136/bmj.320.7237.745
Error, stress, and teamwork in medicine and aviation: cross sectional surveys
Abstract
Objectives: To survey operating theatre and intensive care unit staff about attitudes concerning error, stress, and teamwork and to compare these attitudes with those of airline cockpit crew.
Design: : Cross sectional surveys.
Setting: : Urban teaching and non-teaching hospitals in the United States, Israel, Germany, Switzerland, and Italy. Major airlines around the world.
Participants: : 1033 doctors, nurses, fellows, and residents working in operating theatres and intensive care units and over 30 000 cockpit crew members (captains, first officers, and second officers).
Main outcome measures: : Perceptions of error, stress, and teamwork.
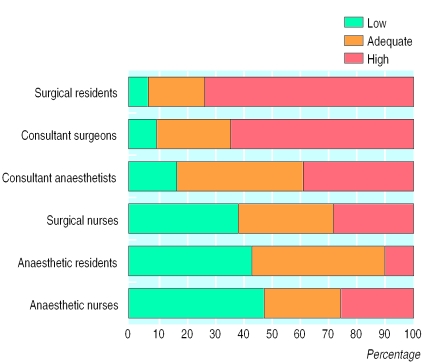
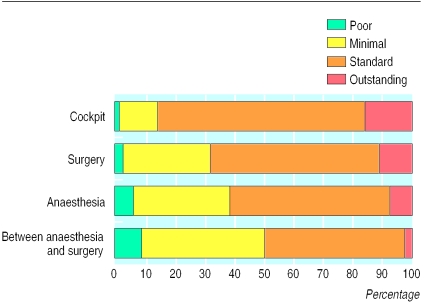
Results: : Pilots were least likely to deny the effects of fatigue on performance (26% v 70% of consultant surgeons and 47% of consultant anaesthetists). Most pilots (97%) and intensive care staff (94%) rejected steep hierarchies (in which senior team members are not open to input from junior members), but only 55% of consultant surgeons rejected such hierarchies. High levels of teamwork with consultant surgeons were reported by 73% of surgical residents, 64% of consultant surgeons, 39% of anaesthesia consultants, 28% of surgical nurses, 25% of anaesthetic nurses, and 10% of anaesthetic residents. Only a third of staff reported that errors are handled appropriately at their hospital. A third of intensive care staff did not acknowledge that they make errors. Over half of intensive care staff reported that they find it difficult to discuss mistakes.
Conclusions: Medical staff reported that error is important but difficult to discuss and not handled well in their hospital. Barriers to discussing error are more important since medical staff seem to deny the effect of stress and fatigue on performance. Further problems include differing perceptions of teamwork among team members and reluctance of senior theatre staff to accept input from junior members.
Figures
References
-
- Thomas EJ, Studdert DM, Burstin HR, Orav EJ, Zeena T, Williams EJ, et al. Incidence and types of adverse events and negligent care in Utah and Colorado. Medical Care (in press). - PubMed
-
- Thomas EJ, Studdert DM, Newhouse JP, Zbar BIW, Howward KM, Williams EJ. Costs of medical injuries in Utah and Colorado. Inquiry. 1999;36:255–264. - PubMed
-
- Leape LL, Lawthers AG, Brennan TA, Johnson WG. Preventing medical injury. Quality Review Bulletin. 1993;19:144–149. - PubMed
-
- Maurino DE, Reason J, Johnston N, Lee RB. Beyond aviation human factors: safety in high technology systems. Brookfield, VT: Ashgate Publishing; 1995.
-
- Leape LL. Error in medicine. JAMA. 1994;272:1851–1857. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical