

Parsonnet score is a good predictor of the duration of intensive care unit stay following cardiac surgery
- PMID: 10722544
- PMCID: PMC1729388
- DOI: 10.1136/heart.83.4.429
Parsonnet score is a good predictor of the duration of intensive care unit stay following cardiac surgery
Abstract
Objective: To investigate the value of the Parsonnet score (PS) in identifying preoperatively patients that are likely to spend < 24 hours on the intensive care unit (ICU) following cardiac surgery.
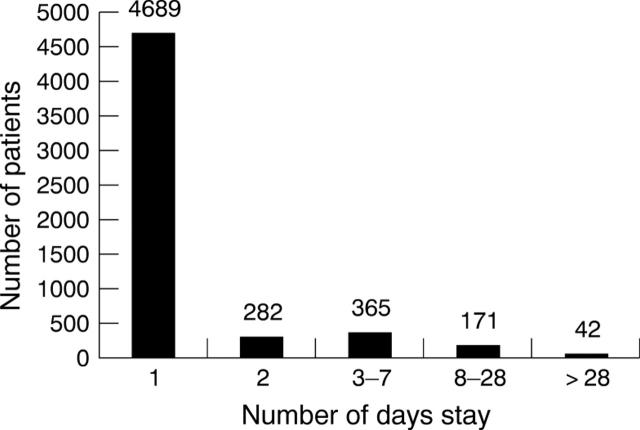
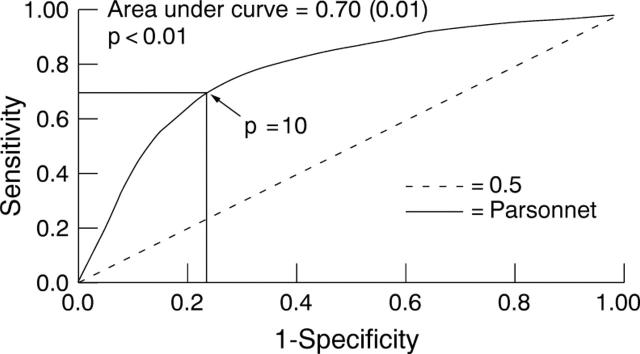
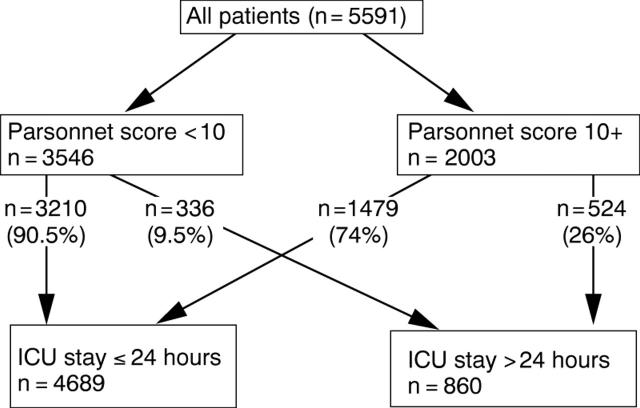
Method: Prospectively collected data on 5591 patients were analysed. PS, mortality, the length of stay on the ICU (ICU-LOS), number of patients with clinical evidence of stroke, need for haemofiltration, resternotomy for bleeding, tracheostomy, and use of intra-aortic balloon pump were documented as outcomes. A receiver operating characteristic (ROC) curve constructed using PS as a predictor of ICU stay < 24 hours identified a PS of 10 as the best cut off point that would predict ICU-LOS < 24 hours. The patients were therefore stratified by PS into two groups, those with a PS of 0 to 9 (PS 0-9) and those with a PS of 10 and above (PS 10+).
Results: The ROC curve constructed using PS as a predictor of ICU stay < 24 hours had an area under the curve of 0.70 (0.01). The maximum efficiency of the test was at a sensitivity of 0.68. This corresponded to PS 10. The positive predictive value of the test at this score was 90.5%. Patients with PS 0-9 had a mean ICU stay of 1.49 days, while patients with PS 10+ had a mean ICU stay of 2.89 days (p = 0.01). The risk of stroke, use of intra-aortic balloon pump, requirement for haemofiltration, need for tracheostomy, and risk of resternotomy for bleeding were each significantly less in patients with PS 0-9 versus those with a score of PS 10+ (p < 0.01 in all cases). The risk of a single complication was 4.7% (PS 0-9) v 15.2% (PS 10+) (p < 0.01).
Conclusion: PS is an impartial and objective method of predicting postoperative complications and ICU stay < 24 hours. This is of value in selecting a cohort of patients likely to maintain a smooth flow of patients through the cardiothoracic unit when resources are limited to a few free ICU beds.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical