

Immediate and long term effects of weight reduction in obese people with asthma: randomised controlled study
- PMID: 10731173
- PMCID: PMC27319
- DOI: 10.1136/bmj.320.7238.827
Immediate and long term effects of weight reduction in obese people with asthma: randomised controlled study
Erratum in
- BMJ 2000 Apr 8;320(7240):984
Abstract
Objective: To investigate the influence of weight reduction on obese patients with asthma.
Design: Open study, two randomised parallel groups.
Setting: Private outpatients centre, Helsinki, Finland.
Participants: Two groups of 19 obese patients with asthma (body mass index (kg/m(2)) 30 to 42) recruited through newspaper advertisements.
Intervention: Supervised weight reduction programme including 8 week very low energy diet.
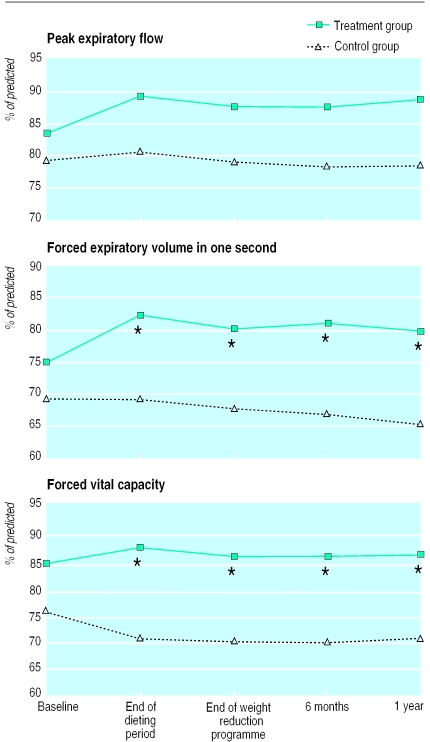
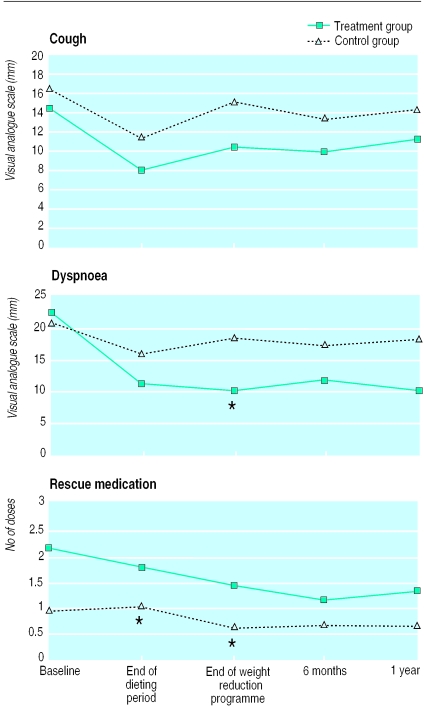
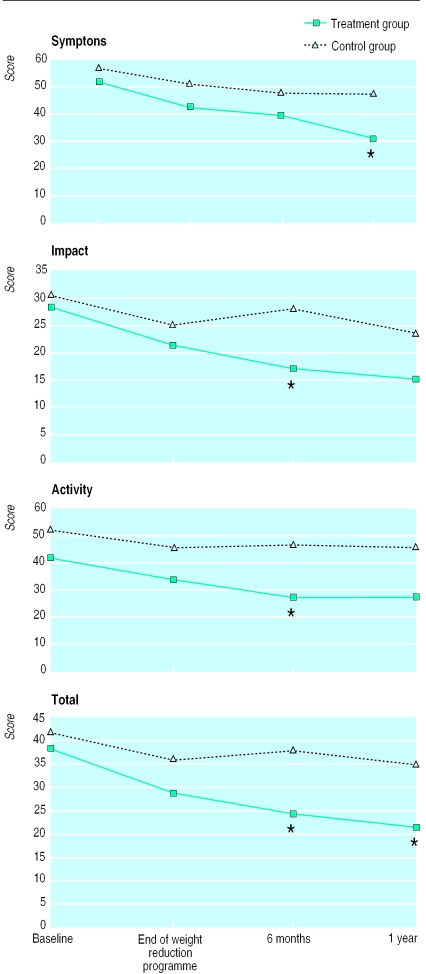
Main outcome measures: Body weight, morning peak expiratory flow (PEF), forced vital capacity (FVC), forced expiratory volume in one second (FEV(1)); and also asthma symptoms, number of acute episodes, courses of oral steroids, health status (quality of life).
Results: At the end of the weight reducing programme, the participants in the treatment group had lost a mean of 14.5% of their pretreatment weight, the controls 0.3%. The corresponding figures after one year were 11.3% and a weight gain of 2.2%. After the 8 week dieting period the difference in changes in percentage of predicted FEV(1) from baseline in the treatment and control groups was 7.2% (95% confidence interval 1.9% to 12.5%, P=0. 009). The corresponding difference in the changes in FVC was 8.6% (4. 8% to 12.5%, P<0.0001). After one year the differences in the changes in the two groups were still significant: 7.6% for FEV(1) (1. 5% to 13.8%, P=0.02) and 7.6% for FVC (3.5% to 11.8%, P=0.001). By the end of the weight reduction programme, reduction in dyspnoea was 13 mm (on a visual analogue scale 0 mm to 100 mm) in the treatment group and 1 mm in the control group (P=0.02). The reduction of rescue medication was 1.2 and 0.1 doses respectively (P=0.03). After one year the differences in the changes between the two groups were -12 for symptom scores (range -1 to -22, P=0.04) and -10 for total scores (-18 to -1, P=0.02). The median number of exacerbations in the treatment group was 1 (0-4) and in the controls 4 (0-7), P=0.001.
Conclusion: Weight reduction in obese patients with asthma improves lung function, symptoms, morbidity, and health status.
Figures
Comment in
- ACP J Club. 2000 Nov-Dec;133(3):103
-
Prevalence of obesity in asthmatic adults.BMJ. 2000 Aug 12;321(7258):448. BMJ. 2000. PMID: 10991591 Free PMC article. No abstract available.
References
-
- Seidell JC, Flegal KM. Assessing obesity: classification and epidemiology. Br Med Bull. 1997;53:238–252. - PubMed
-
- Hakala K, Mustajoki P, Aittomäki J, Sovijärvi ARA. Effect of weight loss and body position on pulmonary function and gas-exchange abnormalities in morbid obesity. Int J Obesity. 1995;19:343–346. - PubMed
-
- Gall H, Gorck G, Kalveram K-J, von Lersner-Lenders S. Soforttypallergie auf Hülsenfrüchte (Leguminosen) [Immediate type allergy to legume food] Allergologie. 1990;13:352–355.
-
- Pekkarinen T, Takala I, Mustajoki P. Two-year maintenance of weight loss after a VLCD and behavioural therapy for obesity: correlation with the scores of questionnaires measuring eating behaviour. Int J Obesity. 1996;20:332–337. - PubMed
-
- Pekkarinen T, Mustajoki P. Comparison of behavioural therapy with and without very low-energy diet in the treatment of morbid obesity. Arch Intern Med. 1997;157:1581–1585. - PubMed