

Intravenous pantoprazole rapidly controls gastric acid hypersecretion in patients with Zollinger-Ellison syndrome
- PMID: 10734021
- PMCID: PMC6736552
- DOI: 10.1016/s0016-5085(00)70139-9
Intravenous pantoprazole rapidly controls gastric acid hypersecretion in patients with Zollinger-Ellison syndrome
Abstract
Background & aims: Parenteral control of gastric acid hypersecretion in conditions such as Zollinger-Ellison syndrome (ZES) or idiopathic gastric acid hypersecretion is necessary perioperatively or when oral medications cannot be taken for other reasons (e.g., during chemotherapy, acute upper gastrointestinal bleeding, or in intensive care unit settings).
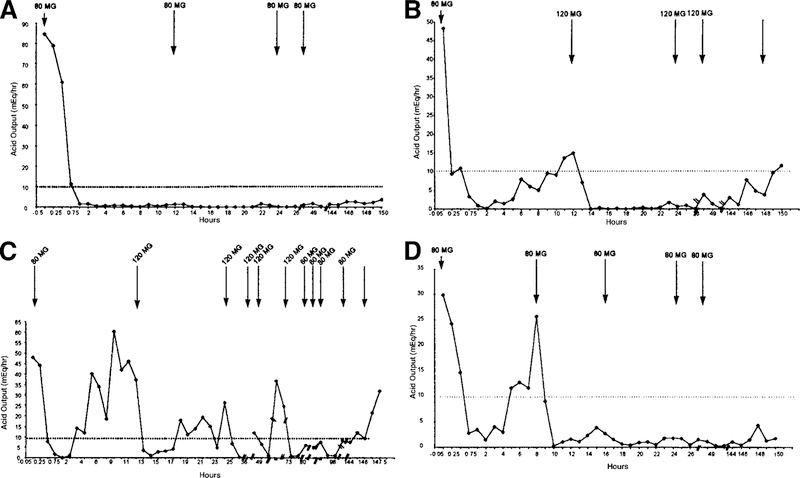
Methods: We evaluated the efficacy and safety of 15-minute infusions of the proton pump inhibitor pantoprazole (80-120 mg every 8-12 hours) in controlling acid output for up to 7 days. Effective control was defined as acid output >10 milliequivalents per hour (mEq/h) (<5 mEq/h in patients with prior acid-reducing surgery) for 24 hours.
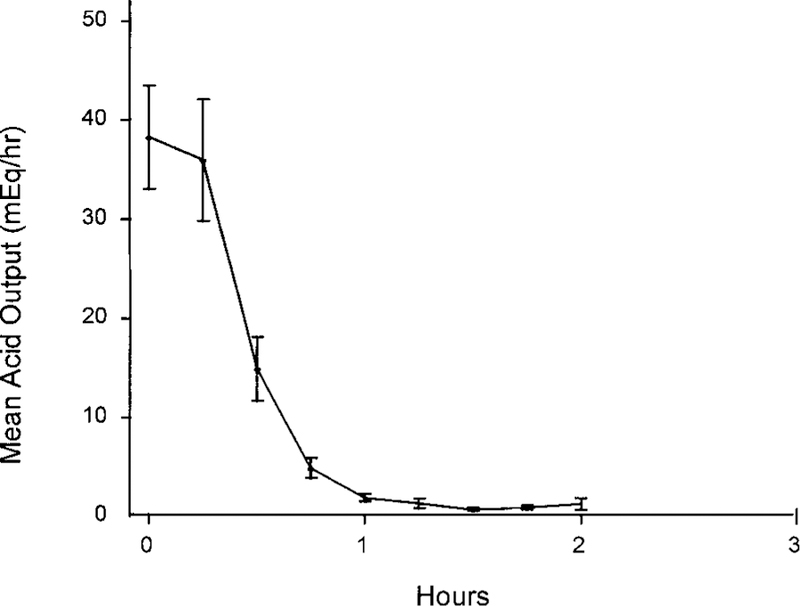
Results: The 21 patients enrolled had a mean age of 51.9 years (range, 29-75) and a mean disease duration of 8.1 years (range, <0.5-21); 13 were male, 7 had multiple endocrine neoplasia syndrome type I, 4 had undergone acid-reducing surgery, 2 had received chemotherapy, and 13 had undergone gastrinoma resections without cure. Basal acid output (mean +/- SD) was 40.2 +/- 27.9 mEq/h (range, 11.2-117.9). In all patients, acid output was controlled within the first hour (mean onset of effective control, 41 minutes) after an initial 80-mg intravenous pantoprazole dose. Pantoprazole, 80 mg every 12 hours, was effective in 17 of 21 patients (81%) for up to 7 days. Four patients required upward dose titration, 2 required 120 mg pantoprazole every 12 hours, and 2 required 80 mg every 8 hours. At study end, acid output remained controlled for 6 hours beyond the next expected dose in 71% of patients (n = 15); mean acid output increased to 4.0 mEq/h (range, 0-9.7). No serious or unexpected adverse events were observed.
Conclusions: Intravenous pantoprazole, 160-240 mg/day administered in divided doses by 15-minute infusion, rapidly and effectively controlled acid output within 1 hour and maintained control for up to 7 days in all ZES patients.
Figures
References
-
- Metz DC, Jensen RT. Endocrine tumors of the pancreas. In: Haubrich WB, Schaffner F, Berk JE, eds. Bockus gastroenterology 5th ed. Volume 4 Philadelphia: Saunders, 1994:3002–3034.
-
- Metz DC. Peptic ulcer disease; diagnosis and treatment. In: DiMarino AJ, Benjamin SB, eds. Gastrointestinal disease: an endoscopic approach Volume 1 Cambridge: Blackwell Science, 1997:285–304.
-
- Zollinger RM, Ellison EC, OíDorisio TM, Sparks J. Thirty years experience with gastrinoma. World J Surg 1984;8:427–435. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
