

doi: 10.1136/gut.44.2008.s1.
An evidence-based appraisal of reflux disease management--the Genval Workshop Report
- PMID: 10741335
- PMCID: PMC1766645
- DOI: 10.1136/gut.44.2008.s1
Item in Clipboard
An evidence-based appraisal of reflux disease management--the Genval Workshop Report
Gut.
1999 Apr.
No abstract available
Figures
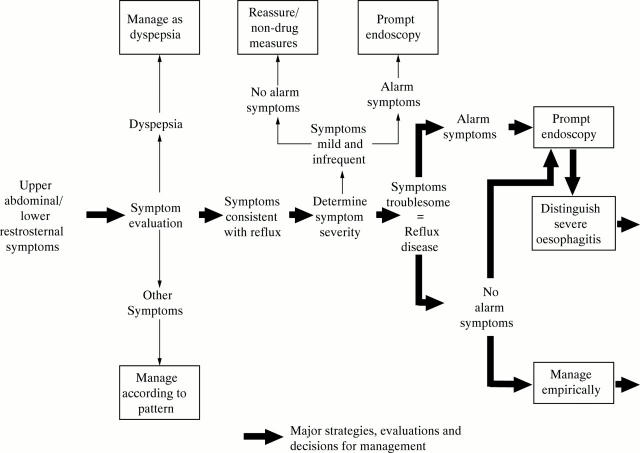
Initial pathways for management of upper abdominal/lower retrosternal symptoms. Patients with reflux disease should be distinguished from individuals who experience mild, infrequent symptoms as a result of gastro-oesophageal reflux (statements 1, 10, 11, and 12). In patients with reflux disease who do not have alarm symptoms there is a lack of data on the relative merits of the strategies of prompt endoscopy, or initial empirical therapy. The Workshop favoured initial endoscopy as most appropriate. The core group was less convinced of this strategy (statement 54). The choice between prompt endoscopy and empirical therapy will, in practice, depend on individual patient factors, as well as access to, and cost of endoscopy (statements 12, 53, 54, and 55).
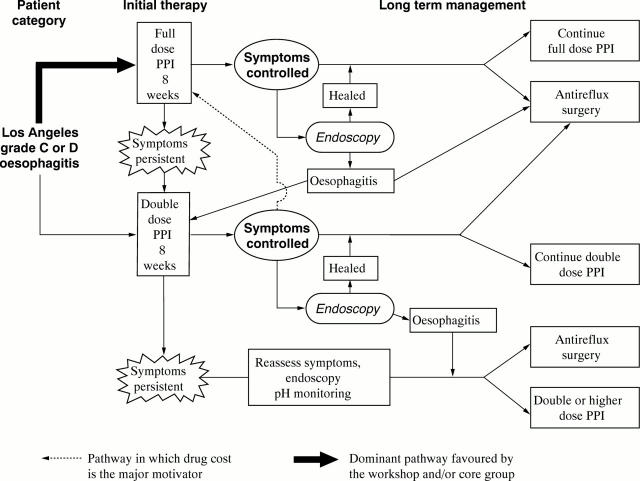
Major management pathways for patients known to have Los Angeles grades C and D oesophagitis. The pathways shown do not take into account the special (and controversial) needs for management of Barrett's oesophagus (statements 28, 29, and 53). Costs are minimised by the use of symptom response for guidance on the success or failure of therapy, rather than endoscopy (statement 62). Symptom control is defined in this setting as the reduction of symptoms to a level that does not impair health related quality of life (statements 11 and 62). For explanation of the exclusive use of proton pump inhibitors (PPI) in this patient category, see the section of text entitled "Management pathways in patients with severe oesophagitis (Los Angeles grades C and D)". Anti-reflux surgery is an appropriate option at any point in the pathway, subject to patient preference and surgeon skill (statements 63-65), but especially should be considered once the patient has been evaluated by initial management strategies.
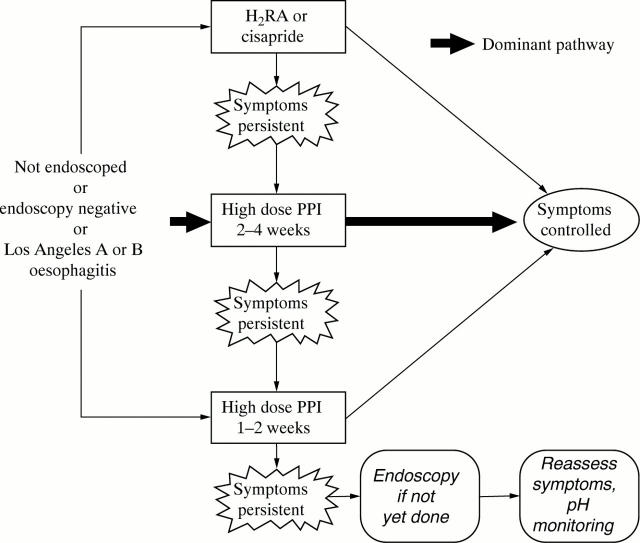
Major management pathways for initial management of patients who have not been endoscoped, and for endoscopy negative or mild oesophagitis patients. For the reasoning behind the use of proton pump inhibitors (PPI) as the dominant initial option, see the section of text entitled "Management pathways in not endoscoped, endoscopy negative or mild oesophagitis (Los Angeles grades A and B) patients". Short term management is primarily determined by whether symptoms are controlled successfully by therapy. Successful control of symptoms is defined as the reduction of symptoms to a level that does not impair health related quality of life (statements 11 and 62). Failure of drug therapy, especially PPI, is an indication for endoscopy in those who have not had this previously.
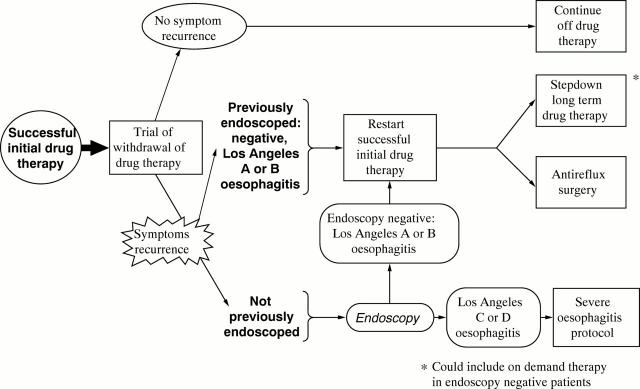
Major management pathways following initial drug therapy that produces successful control of symptoms in the patient groups shown. The pathways ensure that reflux disease is a recurrent problem before long term drug therapy or surgery are considered. The option of on demand therapy merits a trial in patients with endoscopy negative reflux disease, but has been studied relatively little. Non-drug measures are not included in the pathways, in deference to voting on statement 45. However, selected non-drug measures are believed to have some value (see statement 40).
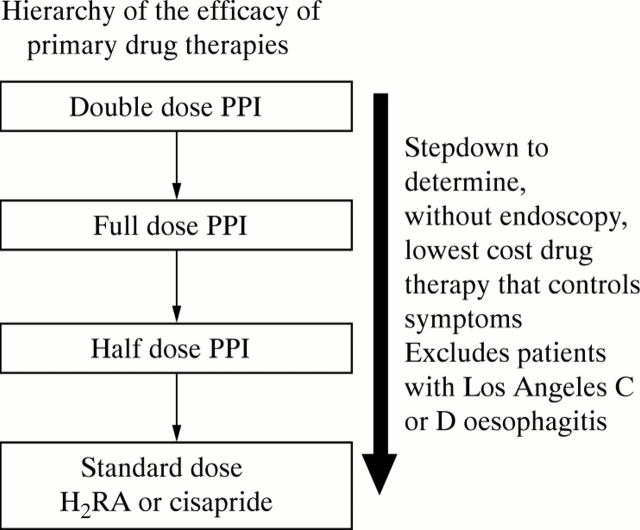
Hierarchy of the efficacy of primary drug treatments, which should be used to guide the choice of step down (or step up) therapy. Drug costs within the applicable practice setting should also guide the choice of step down therapy. Combination H2 receptor antagonist (H2RA) and cisapride therapy are not included as primary therapies, in the light of discussion and voting on statements 51 and 52. Because of the lack of evidence of useful benefit from double dose H2 receptor antagonist and cisapride (see statements 49 and 50) this option has not been included as a mainstream step. PPI, proton pump inhibitor.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical