

Ex vivo and in situ resection of inferior vena cava with hepatectomy for colorectal metastases
- PMID: 10749606
- PMCID: PMC1421021
- DOI: 10.1097/00000658-200004000-00004
Ex vivo and in situ resection of inferior vena cava with hepatectomy for colorectal metastases
Abstract
Objective: To describe the surgical techniques and early results of inferior vena cava (IVC) resection in patients with advanced liver tumors.
Summary background data: Involvement of the IVC by hepatic tumors, although rare, is considered inoperable by standard resection techniques. Concomitant hepatic and IVC resection is required to achieve adequate tumor clearance.
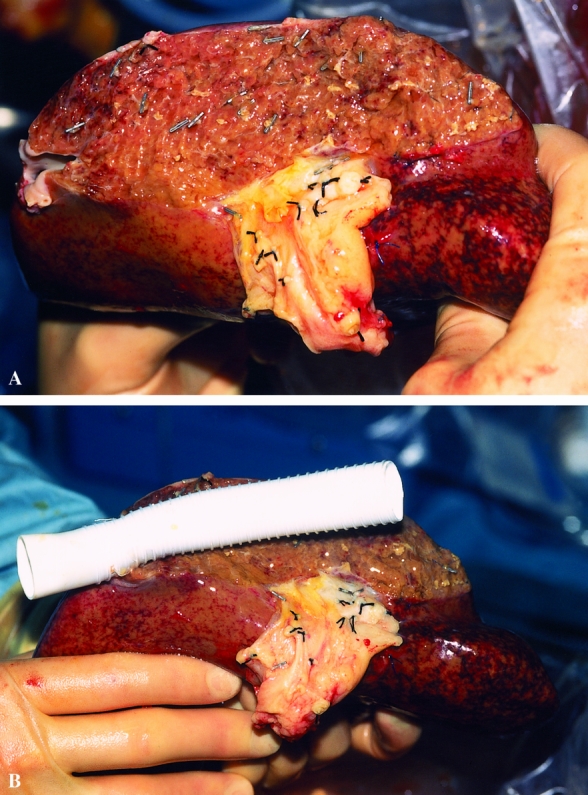
Methods: Between February 1995 and February 1999, 158 patients underwent hepatic resection for colorectal metastases in the authors' unit. Eight patients, aged 42 to 80 years (mean 62 years), with hepatic metastases from colorectal cancer underwent concomitant resection of the IVC and four to six hepatic segments. Resections were carried out under total hepatic vascular exclusion in four patients and ex vivo in four patients. Between 30 degrees and 360 degrees of the retrohepatic IVC was resected and replaced with an autogenous vein patch (n = 1), a ringed Gore-Tex tube graft (n = 2), a Dacron tube graft (n = 1), or a patch (n = 3) or was repaired by primary suturing (n = 1).
Results: There were two early deaths from multiple organ failure. One patient survived 30 months after ex vivo resection but died of renal cell carcinoma, and another died with recurrent disease at 9 months. The remaining four patients remained alive 5 to 12 months after surgery, with no hepatic failure or venous obstruction; tumor recurrence was present in two. Nonthrombotic occlusion of the neocava occurred in one patient and was stented successfully.
Conclusions: Although concomitant hepatic and IVC resection is associated with a considerable surgical risk, this aggressive surgical approach offers hope for patients with hepatic tumors involving the IVC, who would otherwise have a dismal prognosis. This procedure can be performed under total hepatic vascular exclusion, with or without venovenous bypass, and by ex vivo bench resection.
Figures


References
-
- Bengtsson G, Carlsson G, Hafstrom L, Jonsson P. Natural history of patients with untreated liver metastases from colorectal cancer. Am J Surg 1981; 141:586–589. - PubMed
-
- Lahr CJ, Soong S-J, Cloud G, et al. A multifactorial analysis of prognostic factors in patients with liver metastases from colorectal carcinoma. J Clin Oncol 1983; 1:720–726. - PubMed
-
- Rougier P, Milan C, Lazoethes F, et al. Prospective study of prognostic factors in patients with unresected hepatic metastases from colorectal cancer. Br J Surg 1995; 82:1397–1400. - PubMed
-
- Isenberg J, Fischbach R, Kruger I, Keller HW. Treatment of liver metastases from colorectal cancer. Anticancer Res 1996; 16:1291–1295. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
