

Effect of reresection in extremity soft tissue sarcoma
- PMID: 10767786
- PMCID: PMC1421052
- DOI: 10.1097/00000658-200005000-00005
Effect of reresection in extremity soft tissue sarcoma
Abstract
Objective: To determine whether reresection affects survival in patients with inadequately resected, primary extremity soft tissue sarcoma. This study correlates reresection with local recurrence-free survival, metastasis-free survival, and disease-free survival.
Summary background data: Soft tissue sarcomas are rare neoplasms, with an incidence of approximately 6,000 per year in the United States. Because these tumors are rare and benign soft tissue tumors are common, many are initially thought to be benign and are excised without wide margins.
Methods: Patients who underwent treatment for primary tumors from July 1982 to June 1999 at a single institution were the subject of study. Two groups of patients were analyzed: those who underwent one definitive resection (one operation) and those whose tumors were previously resected and who were then referred for subsequent reresection (two operations). Patients were given adjuvant radiation or chemotherapy according to the standard of care.
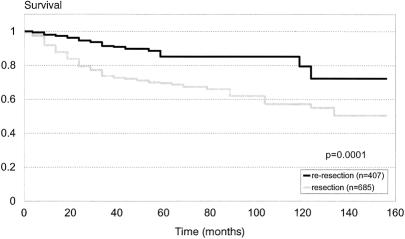
Results: Of 1,092 patients with primary extremity soft tissue sarcoma underwent resection, 685 underwent definitive radical resection and 407 underwent reresection after undergoing excisional resection elsewhere. Median follow-up was 4.8 years. The 5-year disease-free survival rate of the definitive resection (one operation) group was 70%; that of the reresection (two operations) group was 88%. On multivariate analysis, reresection was adjusted and controlled for age, grade, depth, size, histology, and margins. Reresection remained a significant predictor of improved disease-free survival, even after these adjustments. To determine whether this difference was stage- or referral-biased, the patient population was divided by AJCC stage. In all stages there was a trend toward improved outcome; this was most marked for those with stage III disease (>5 cm, high-grade, and deep).
Conclusions: Patients with extremity soft tissue sarcoma who undergo reresection with two "primary" operations have an improved survival compared with those who undergo one operation. The most plausible explanation, referral and selection bias, is questionable given the significance of reresection as a variable after adjusting for stage and other risk factors. This suggests that where indicated and possible, reresection should be liberally applied in patients with primary extremity soft tissue sarcoma.
Figures


References
-
- Lewis JJ, Brennan MF. Soft tissue sarcomas. In: Sabiston DC, ed. The Biological Basis of Modern Surgical Practice. New York: Saunders; 1999: 528–534.
-
- Gustafson P, Dreinhofer KE, Rydholm A. Soft tissue sarcoma should be treated at a tumor center. A comparison of quality of surgery in 375 patients. Acta Orthop Scand 1994; 65:47–50. - PubMed
-
- Gustafson P. Soft tissue sarcoma. Epidemiology and prognosis in 508 patients. Acta Orthop Scand 1994; 259(suppl):1–31. - PubMed
-
- Clasby R, Tilling K, Smith MA, Fletcher CDM. Variable management of soft tissue sarcoma: regional audit with implications for specialist care. Br J Surg 1997; 84:1692–1696. - PubMed
-
- Hajdu SI, Shiu MH, Brennan MF. The role of the pathologist in the management of soft tissue sarcomas. World J Surg 1988; 12:326–331. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
