

Effect of minimally invasive radioguided parathyroidectomy on efficacy, length of stay, and costs in the management of primary hyperparathyroidism
- PMID: 10767795
- PMCID: PMC1421061
- DOI: 10.1097/00000658-200005000-00014
Effect of minimally invasive radioguided parathyroidectomy on efficacy, length of stay, and costs in the management of primary hyperparathyroidism
Abstract
Objective: To compare the first 20 patients who underwent minimally invasive radioguided parathyroidectomies (MIRPs) performed at the authors' institution with 20 similar patients who underwent a more conventional surgical approach for primary hyperparathyroidism.
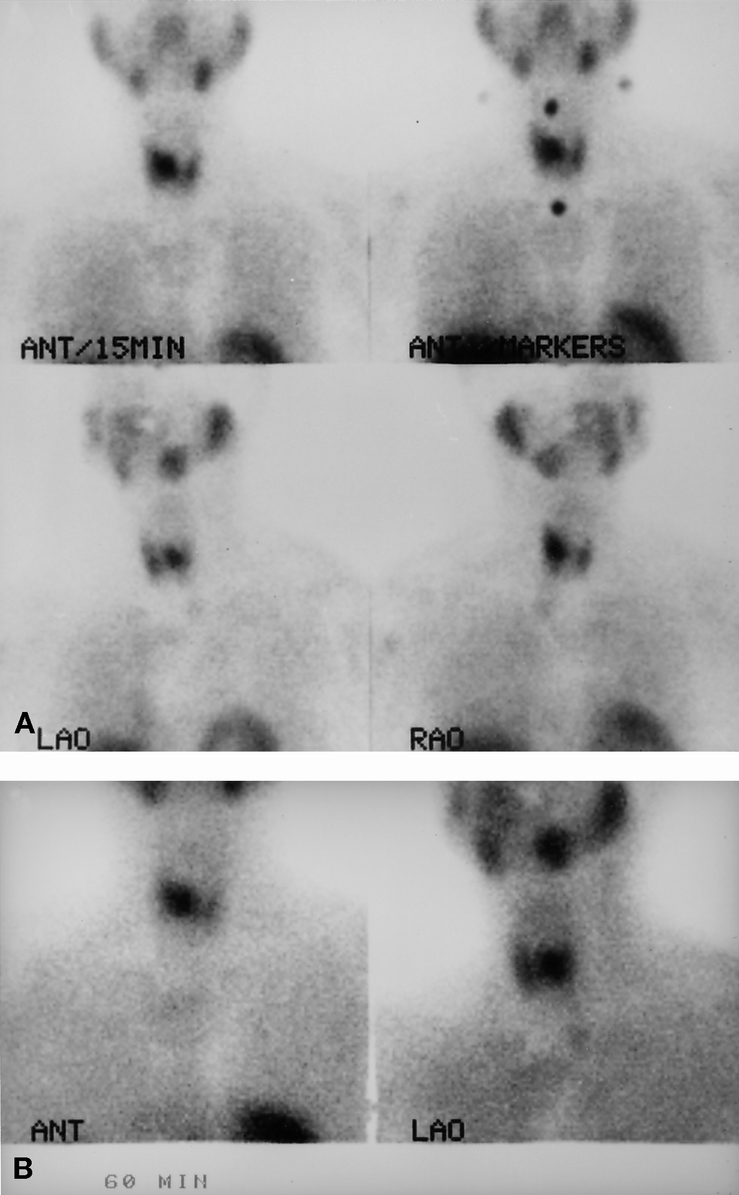
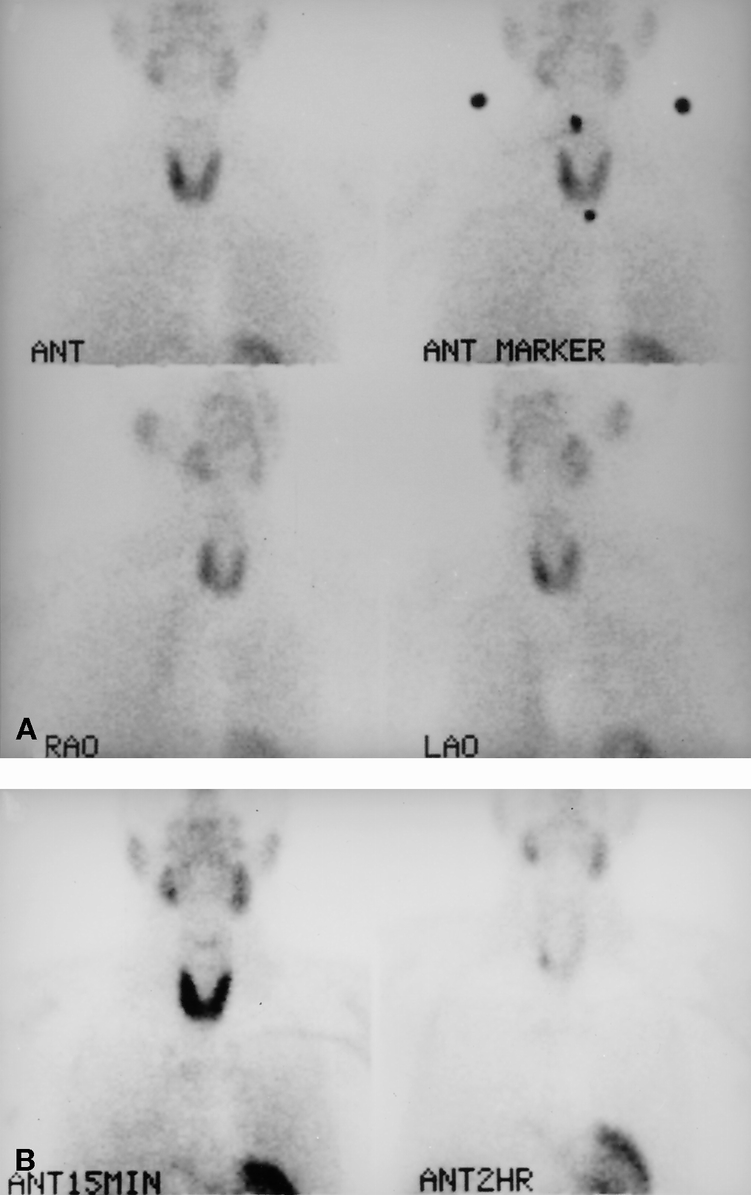
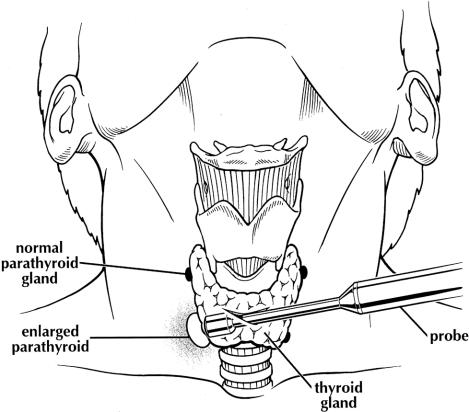
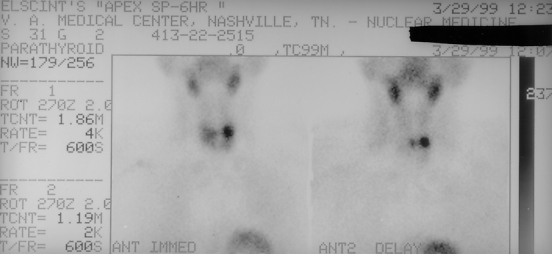
Summary background data: The technique of parathyroidectomy has traditionally involved a bilateral exploration of the neck with the intent of visualizing four parathyroid glands and resecting enlarged parathyroid glands. Parathyroid scanning using radioisotopes has evolved and now can localize adenomas in 80% to 90% of patients. MIRP combines parathyroid scanning with a hand-held intraoperative detector that guides the surgeon to the adenoma.
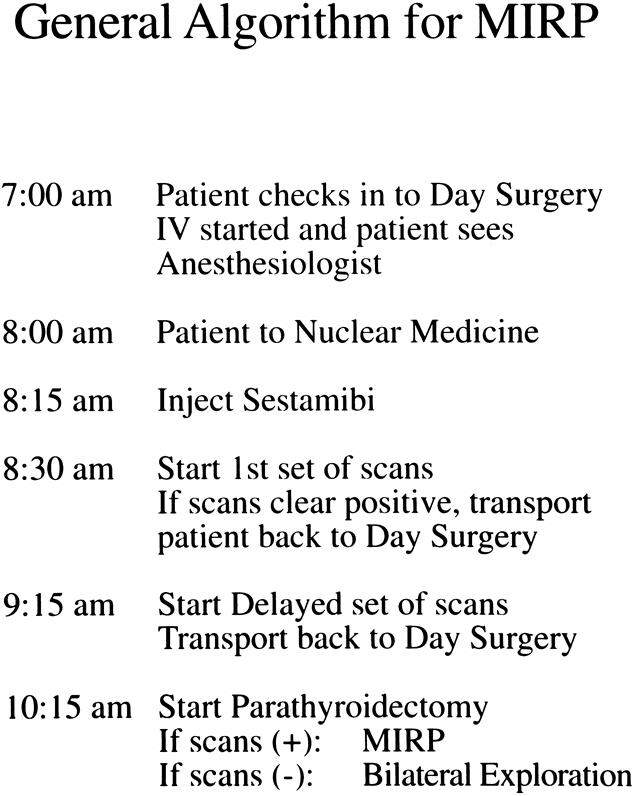
Methods: Forty patients with documented primary hyperparathyroidism who underwent surgery by a single surgeon between January 1998 and May 1999 were included in this study. Twenty of these patients underwent MIRP. The technique involved injecting 20 mCi technetium-99m sestamibi 2 hours before surgery and performing a parathyroid scan. If the scan was considered positive for a single adenoma, patients were taken to the operating room and given the choice of either general anesthesia or intravenous sedation with local anesthesia. Using an incision of 4 cm or less, the dissection down to the adenoma was guided by the Navigator miniature hand-held probe. An additional 20 patients who underwent more conventional bilateral or unilateral neck exploration were chosen to match the MIRP patient population. Both groups included four patients undergoing repeat surgery for persistent or recurrent primary hyperparathyroidism and one patient with multiple endocrine neoplasia type 1 syndrome. Patient demographics, preoperative calcium and parathyroid hormone levels, operative time, total time in the operating room, time in the recovery room, complications, hospital charges for the operating room, and total hospital charges were analyzed.
Results: There were no differences in patient demographics, presenting symptoms, or preoperative calcium level between patients undergoing the standard procedure versus MIRP. Operative time, total time in the operating room, operative charges, and total hospital charges were significantly reduced in the MIRP group. All 40 patients were cured of primary hyperparathyroidism. There were no recurrent laryngeal nerve injures in either group. The mean length of stay in the standard group was 1. 35 days; in the MIRP group, 65% of patients were discharged within 5 hours after surgery.
Conclusions: The MIRP technique resulted in excellent cure rates for primary hyperparathyroidism while simultaneously decreasing operative time and hospital stays. These resulted in significant cost reductions without compromising patient safety. The technique may significantly change the management of primary hyperparathyroidism.
Figures
References
-
- Melton LJ III. Epidemiology of primary hyperparathyroidism. J Bone Min Res 1991; 6:S25–S29. - PubMed
-
- Heath H III, Hodgson SF, Kenneday MA. Primary hyperparathyroidism: incidence, morbidity, and potential economic impact in a community. N Engl J Med 1980 302:189–193. - PubMed
-
- Ljunghall S, Hellman P, Rastad J, Akerstrom G. Primary hyperparathyroidism: epidemiology, diagnosis and clinical picture. World J Surg 1991; 15:681–687. - PubMed
-
- Auguste L-J, Attie JN, Schnaap D. Initial failure of surgical exploration in patients with primary hyperparathyroidism. Am J Surg 1990; 160:333–336. - PubMed
-
- van Heerden JA, Grant CS. Surgical treatment of primary hyperparathyroidism: an institutional perspective. World J Surg 1991; 15:688–692. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
