

Review
doi: 10.1136/heart.83.5.588.
Arrhythmogenic right ventricular cardiomyopathy: diagnosis, prognosis, and treatment
Affiliations
- PMID: 10768917
- PMCID: PMC1760807
- DOI: 10.1136/heart.83.5.588
Item in Clipboard
Review
Arrhythmogenic right ventricular cardiomyopathy: diagnosis, prognosis, and treatment
Heart.
2000 May.
No abstract available
Figures
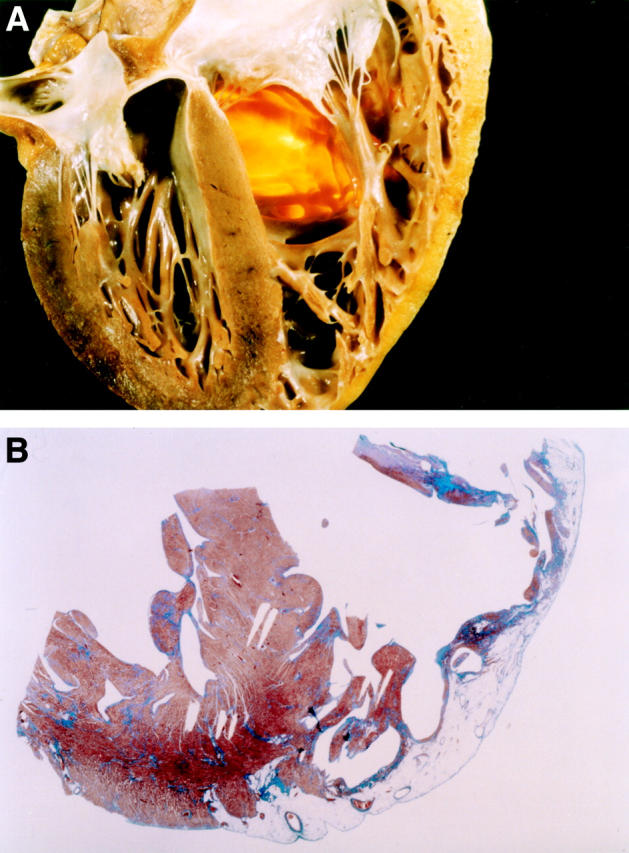
Morphologic features in a 25 year old man who died suddenly from arrhythmogenic right ventricular cardiomyopathy. (A) Four chamber view cut of the heart specimen showing the transmural fatty replacement of the right ventricular free wall and the translucent infundibulum. (B) Panoramic histologic view of the same heart confirming that the myocardial atrophy is confined to the right ventricle and substantially spares the interventricular septum as well as the left ventricular free wall (trichrome Heidenhain × 3). Reproduced from Basso C, Corrado D, Rossi L, et al. Morbid anatomy. In: Nava A, Rossi L, Thiene G, eds. Arrhythmogenic right ventricular cardiomyopathy—dysplasia. Elsevier, Amsterdam 1997, pp 71-86, with permission of the publisher.
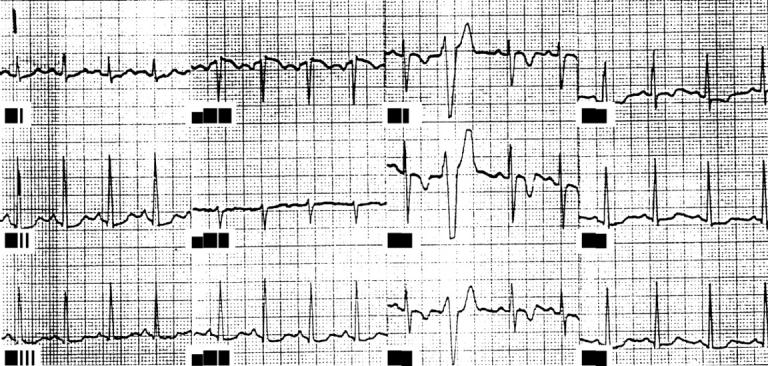
Twelve lead ECG obtained at preparticipation screening in a 19 year old football player who subsequently died from ARVC during a competitive game. Note the typical abnormalities consisting of inverted T waves from V1 to V4 and isolated premature ventricular beats with an LBBB morphology.
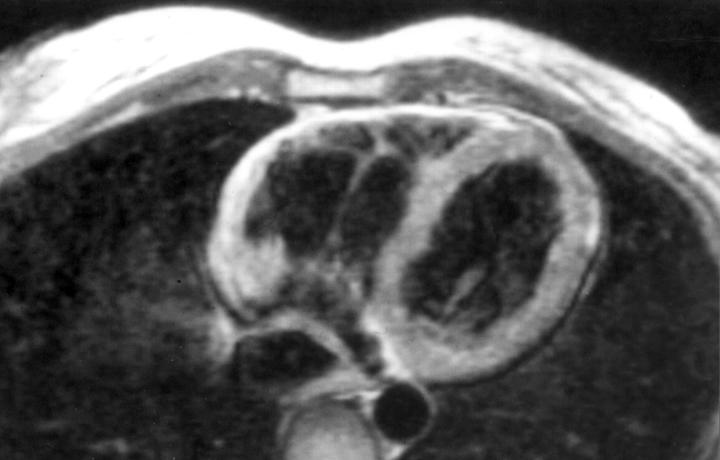
MRI findings in a 22 year old woman with a history of dizziness and sustained ventricular tachycardia with an LBBB pattern. Short axis view showing a dilated right ventricle with a brighter signal from a thin anterior free wall. Reproduced from Menghetti L, Basso C, Nava A, et al. Spin-echo nuclear magnetic resonance for tissue characterisation in arrhythmogenic right ventricular cardiomyopathy. Heart 1996;76:467-70, with permission of the publisher.
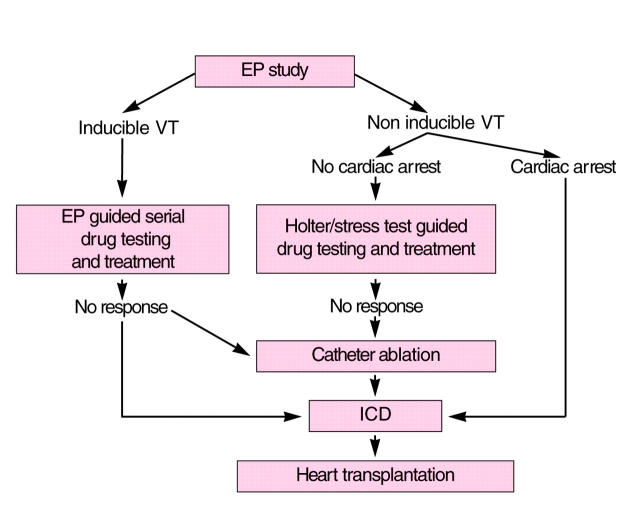
Treatment strategy in ARVC complicated by VT/VF.
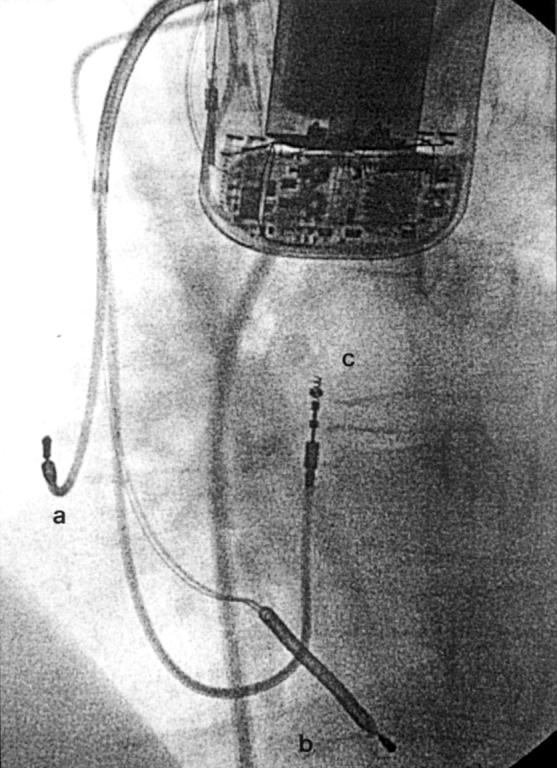
A 24 year old man affected by ARVC complicated by severe ventricular arrhythmias, with a recent family history of sudden death. (A) Twelve lead ECG during programmed ventricular stimulation: the first two beats at sinus rhythm show a low voltage QRS complex in the peripheral leads and T wave inversion in right precordial leads. After a drive of five paced ventricular beats, three extrastimuli induce a sustained ventricular tachycardia with an LBBB pattern and a cycle length of 250 ms, which was promptly interrupted by DC shock caused by the rapid haemodynamic deterioration. Serial antiarrhythmic drug testing, including sotalol, failed to identify any effective drug. (B) Chest radiography (60° left anterior oblique) of the same patient after implantation of a transvenous prophylactic automatic cardioverter defibrillator. Besides the atrial lead (a) and the double coil ventricular lead (b) for cardioversion, a third lead (c) was screwed onto the mid septum to assure a reliable sensing and pacing function. A B
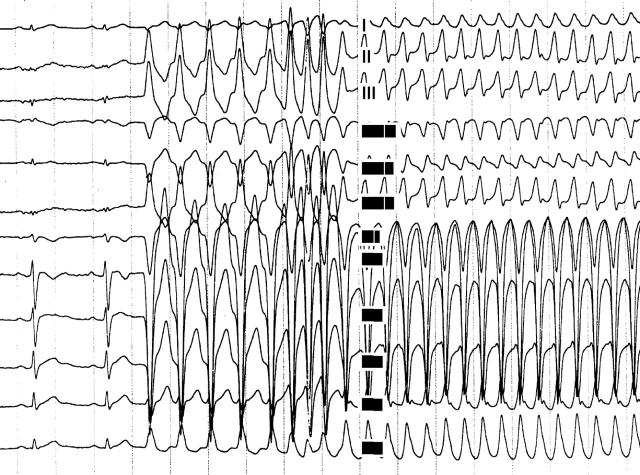
A 24 year old man affected by ARVC complicated by severe ventricular arrhythmias, with a recent family history of sudden death. (A) Twelve lead ECG during programmed ventricular stimulation: the first two beats at sinus rhythm show a low voltage QRS complex in the peripheral leads and T wave inversion in right precordial leads. After a drive of five paced ventricular beats, three extrastimuli induce a sustained ventricular tachycardia with an LBBB pattern and a cycle length of 250 ms, which was promptly interrupted by DC shock caused by the rapid haemodynamic deterioration. Serial antiarrhythmic drug testing, including sotalol, failed to identify any effective drug. (B) Chest radiography (60° left anterior oblique) of the same patient after implantation of a transvenous prophylactic automatic cardioverter defibrillator. Besides the atrial lead (a) and the double coil ventricular lead (b) for cardioversion, a third lead (c) was screwed onto the mid septum to assure a reliable sensing and pacing function. A B
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources