

Preservation of myocardial beta-adrenergic receptor signaling delays the development of heart failure after myocardial infarction
- PMID: 10779554
- PMCID: PMC25845
- DOI: 10.1073/pnas.090091197
Preservation of myocardial beta-adrenergic receptor signaling delays the development of heart failure after myocardial infarction
Abstract
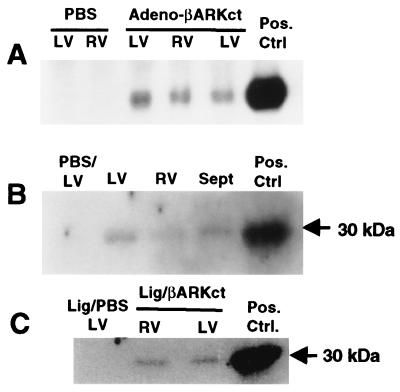
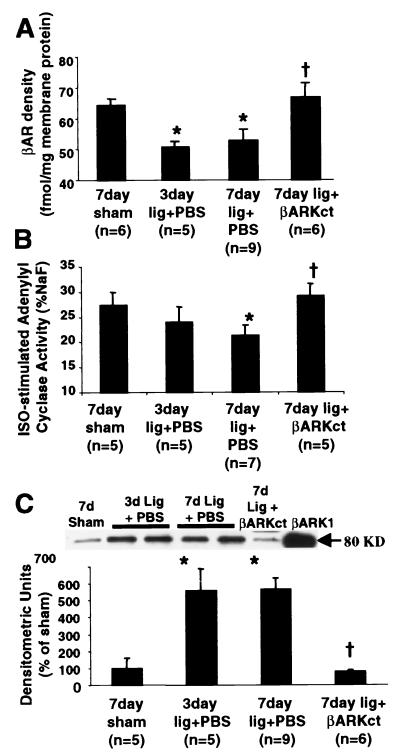
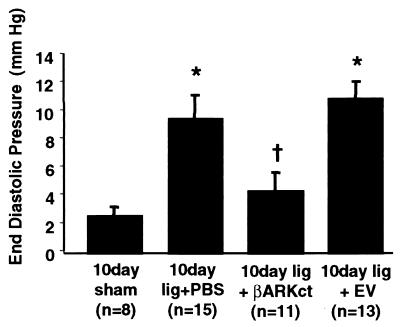
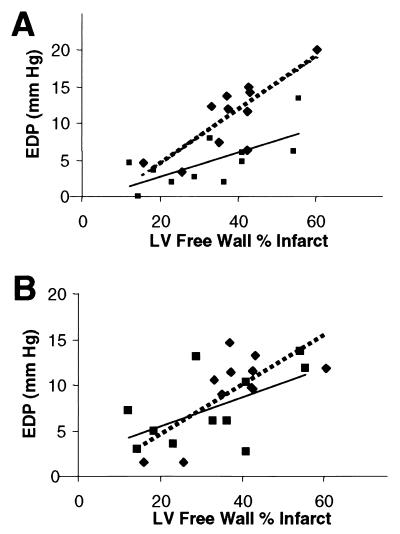
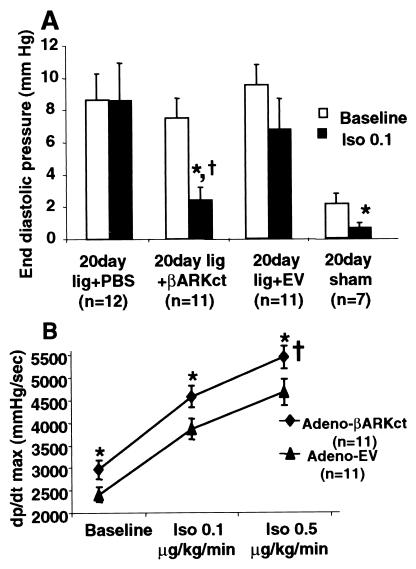
When the heart fails, there is often a constellation of biochemical alterations of the beta-adrenergic receptor (betaAR) signaling system, leading to the loss of cardiac inotropic reserve. betaAR down-regulation and functional uncoupling are mediated through enhanced activity of the betaAR kinase (betaARK1), the expression of which is increased in ischemic and failing myocardium. These changes are widely viewed as representing an adaptive mechanism, which protects the heart against chronic activation. In this study, we demonstrate, using in vivo intracoronary adenoviral-mediated gene delivery of a peptide inhibitor of betaARK1 (betaARKct), that the desensitization and down-regulation of betaARs seen in the failing heart may actually be maladaptive. In a rabbit model of heart failure induced by myocardial infarction, which recapitulates the biochemical betaAR abnormalities seen in human heart failure, delivery of the betaARKct transgene at the time of myocardial infarction prevents the rise in betaARK1 activity and expression and thereby maintains betaAR density and signaling at normal levels. Rather than leading to deleterious effects, cardiac function is improved, and the development of heart failure is delayed. These results appear to challenge the notion that dampening of betaAR signaling in the failing heart is protective, and they may lead to novel therapeutic strategies to treat heart disease via inhibition of betaARK1 and preservation of myocardial betaAR function.
Figures
References
-
- Brodde O E. Pharmacol Ther. 1993;60:405–430. - PubMed
-
- Leimbach W N, Wallin G, Victor R G, Aylward P E, Sundlof G, Mark A L. Circulation. 1986;73:913–919. - PubMed
-
- Bristow M R, Ginsburg R, Minobe W, Cubicciotti R, Sageman W S, Lurie K, Billingham M E, Harrison D C, Stinson E B. N Engl J Med. 1982;307:205–211. - PubMed
-
- Ungerer M, Bohm M, Elce J S, Erdmann E, Lohse M L. Circulation. 1993;87:454–463. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
