

Human herpesvirus 8 infections in the Amsterdam Cohort Studies (1984-1997): analysis of seroconversions to ORF65 and ORF73
- PMID: 10781089
- PMCID: PMC18319
- DOI: 10.1073/pnas.97.9.4838
Human herpesvirus 8 infections in the Amsterdam Cohort Studies (1984-1997): analysis of seroconversions to ORF65 and ORF73
Abstract
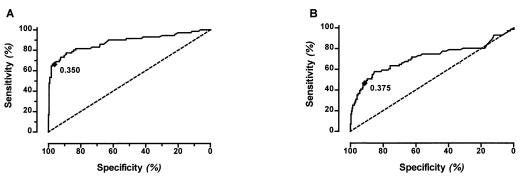
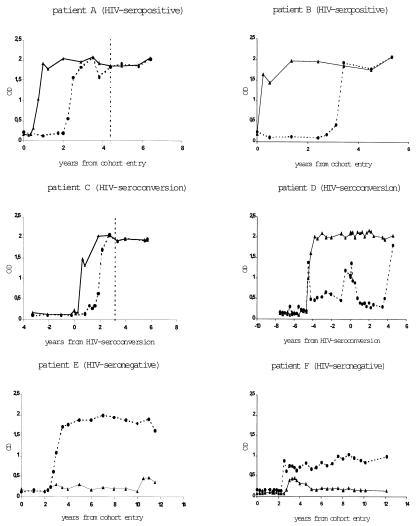
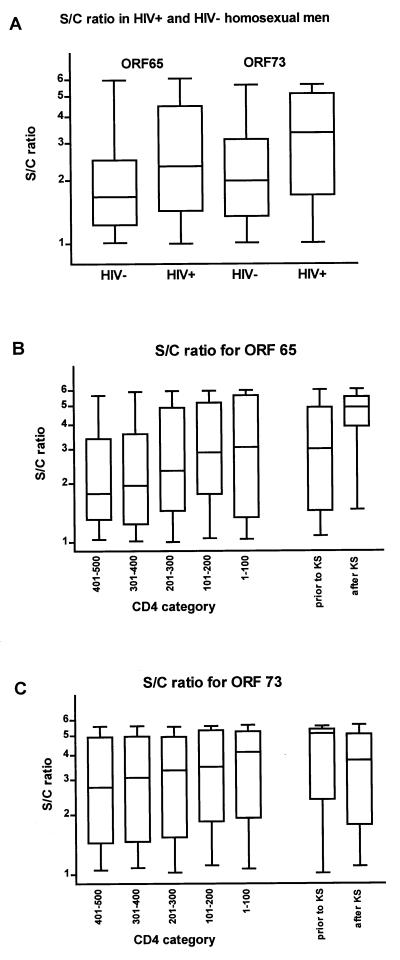
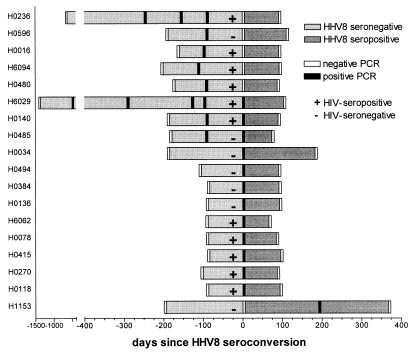
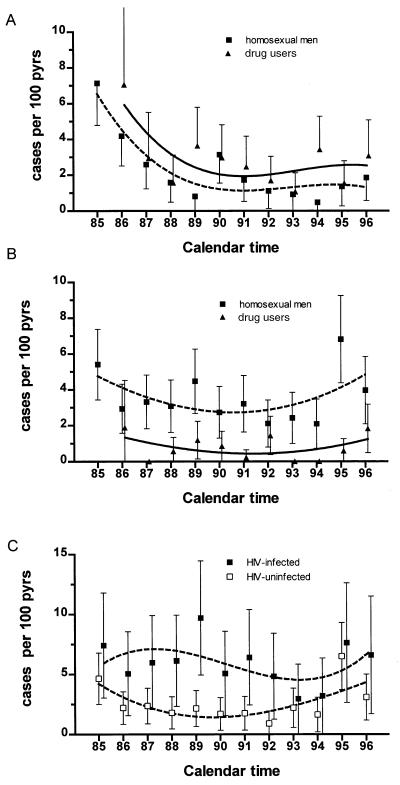
We have shown previously that human herpesvirus 8 (HHV8) seroconversion for antibodies to the latency-associated nuclear antigen encoded by ORF73 and/or the lytic capsid antigen (vp19) encoded by ORF65 is associated with orogenital contact and is strongly linked to the development of Kaposi's sarcoma among HIV-infected individuals in the Amsterdam Cohort Studies. Here, we investigate the relationship between seroconversion to these antigens and primary HHV8 infection. Between 1984 and 1997, 215 HHV8 seroconversions to ORF73 (106 cases or 49%) and/or to ORF65 (159 cases or 74%) were recorded in the cohort of homosexual men. The HHV8 seroconversion rate among HIV-infected homosexual men (6.2 per 100 person years) was consistently higher than among HIV-uninfected men (2.6 per 100 person years). In HIV-infected but not in uninfected individuals, seroconversion to ORF73/latency-associated nuclear antigen precedes that to ORF65/vp19. Antibody levels to both ORF65- and ORF73-encoded antigens were higher in HIV-infected than in HIV-uninfected men, and among HIV-seropositives, antibody levels to ORF65/vp19 rise even higher with declining CD4 cell counts and peak with Kaposi's sarcoma development, suggesting continuing and increasing viral replication. In 10.3% of HHV8 seroconversions, transient serum viremia could be demonstrated before or at seroconversion. Together with the previously reported link between unprotected orogenital sex and HHV8 seroconversion, our observations suggest that HHV8 seroconversions result from primary infections.
Figures
References
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
