

Scientific, ethical, and logistical considerations in introducing a new operation: a retrospective cohort study from paediatric cardiac surgery
- PMID: 10784538
- PMCID: PMC27358
- DOI: 10.1136/bmj.320.7243.1168
Scientific, ethical, and logistical considerations in introducing a new operation: a retrospective cohort study from paediatric cardiac surgery
Abstract
Objective: To review the initial impact on mortality of infants with congenital heart disease of a new surgical technique that is now taken for granted.
Design: Retrospective cohort study.
Setting: A tertiary paediatric cardiology centre.
Subjects: 325 consecutive neonates with simple transposition of the great arteries admitted before, during, and after the preferred management changed from the Senning operation to the arterial switch (1978-98); and 100 consecutive neonates requiring a different neonatal open heart operation that did not change in that period.
Main outcome measures: Mortality before and early after operation reconstructed sequentially as the series evolved and retrospectively once the series was complete; actuarial survival associated with the different treatment strategies.
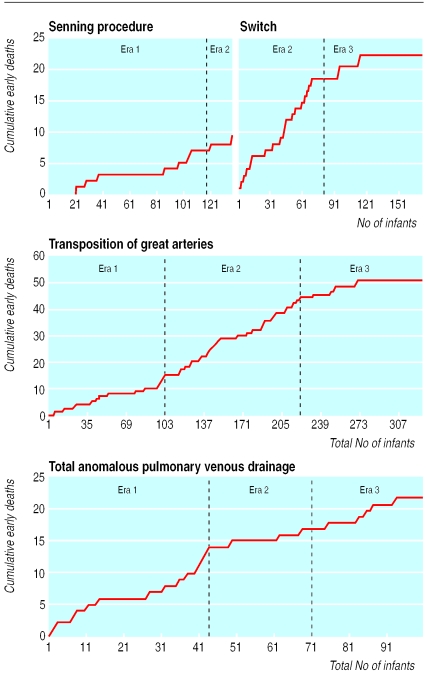
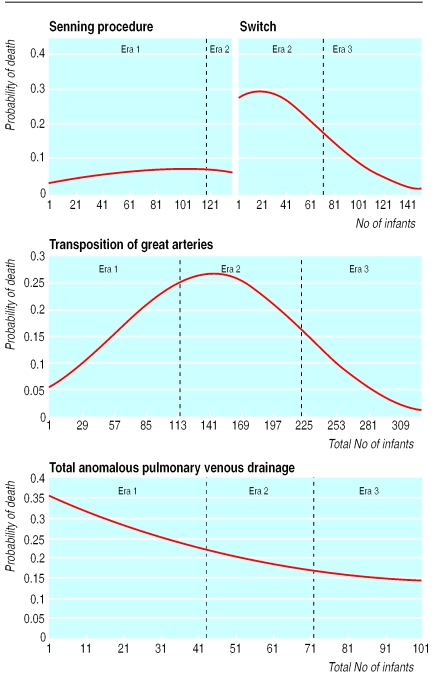
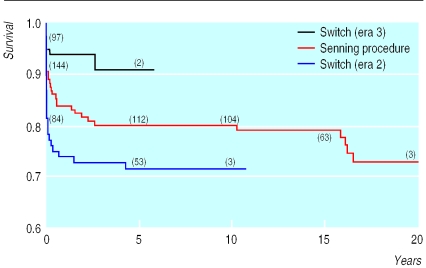
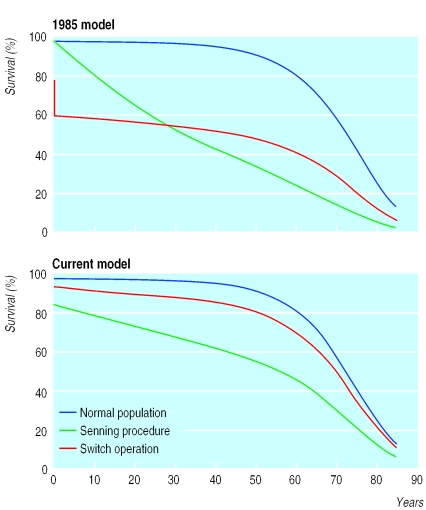
Results: For both the transposition and the comparison group, early mortality in 1998 was lower than in 1978. During that period, however, there was a phase temporally related to the adoption of the switch operation in which early mortality for transposition increased. Actuarial survival of recent patients with "intention to treat" with arterial switch is superior to those with intention to treat with the Senning operation, as predicted when the switch operation was first adopted.
Conclusions: A period of increased hazard for individual patients may occur when a specialist community, a particular unit, and an individual surgeon are all learning a new technique concurrently. Obtaining informed consent during this time of uncertainty is helped by clarity about the objectives of treatment and availability of relevant local and international data.
Figures
References
-
- Jatene AD, Fontes VF, Paulista PP, Souza LCB, Neger F, Galantier M, et al. Successful anatomic correction of transposition of the great vessels: a preliminary report. Arquivos Brasilieros de Cardiologia. 1975;28:461–462. - PubMed
-
- Castaneda AR, Trusler GA, Paul MH, Blackstone EH, Kirklin JW the Congenital Heart Surgeons Society. The early results of treatment of simple transposition in the current era. J Thorac Cardiovasc Surg. 1988;95:14–28. - PubMed
-
- Macartney FJ, Spiegelhalter DJ, Rigby ML. Medical management. In: Anderson RH, Macartney FJ, Shinebourne EA, Tynan M, editors. Paediatric cardiology. Edinburgh: Churchill Livingstone; 1987. pp. 421–422.
-
- DeLeval M, Francois K, Bull C, Brawn W, Spiegelhalter DJ. Analysis of a cluster of surgical failures. J Thorac Cardiovasc Surg. 1994;107:914–924. - PubMed
-
- Sarkar D, Bull C, Yates R, Wright D, Cullen S, Gewellig M, et al. Comparison of long term outcomes of atrial repair of simple transposition with implications for an arterial switch strategy. Circulation. 1999;100(part III):76–81. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical