

Imaging of mucormycosis skull base osteomyelitis
- PMID: 10815656
- PMCID: PMC7976772
Imaging of mucormycosis skull base osteomyelitis
Abstract
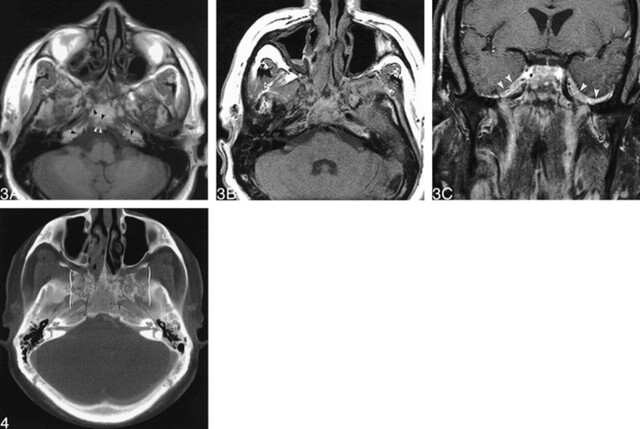
Skull base osteomyelitis (SBO) is typically bacterial in origin and caused by Pseudomonas, although the fungus Aspergillus has also rarely been implicated. SBO generally arises from ear infections and infrequently complicates sinonasal infection. Rhinocerebral Mucor infection is characteristically an acute, fulminant, and deadly infection also affecting the orbits and deep face and is associated with intracranial complications. Bony involvement is uncommon because of the angioinvasive nature of the fungus. More recently, chronic invasive Mucor sinusitis has been described. We report the unusual clinical and imaging features of a patient with biopsy-proven invasive mucormycosis arising from chronic isolated sphenoid sinus disease, who presented with extensive SBO and a paucity of deep facial, orbital, or intracranial involvement.
Figures

References
-
- Chandler JR, Grobman L, Quencer R, et al. Osteomyelitis of the base of the skull. Laryngoscope 1986;96:245-251 - PubMed
-
- Grobman LR, Ganz W, Casiano R, Goldberg S. Atypical osteomyelitis of the skull base. Laryngoscope 1989;99:671-676 - PubMed
-
- Murray ME, Britton J. Osteomyelitis of the skull base: the role of high resolution CT in diagnosis. Clin Radiology 1994;49:408-411 - PubMed
-
- Senegor M, Lewis HP. Samonella osteomyelitis of the skull base. Surg Neurol 1991;36:37-39 - PubMed
-
- Hoistad DL, Duvall AJ. Sinusitis with contiguous abscess involvement of the clivus and petrous apices. Ann Otol Rhinol Laryngol 1999;108:463-466 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical