

Dynamic contrast-enhanced T2-weighted MR imaging of recurrent malignant gliomas treated with thalidomide and carboplatin
- PMID: 10815664
- PMCID: PMC7976741
Dynamic contrast-enhanced T2-weighted MR imaging of recurrent malignant gliomas treated with thalidomide and carboplatin
Abstract
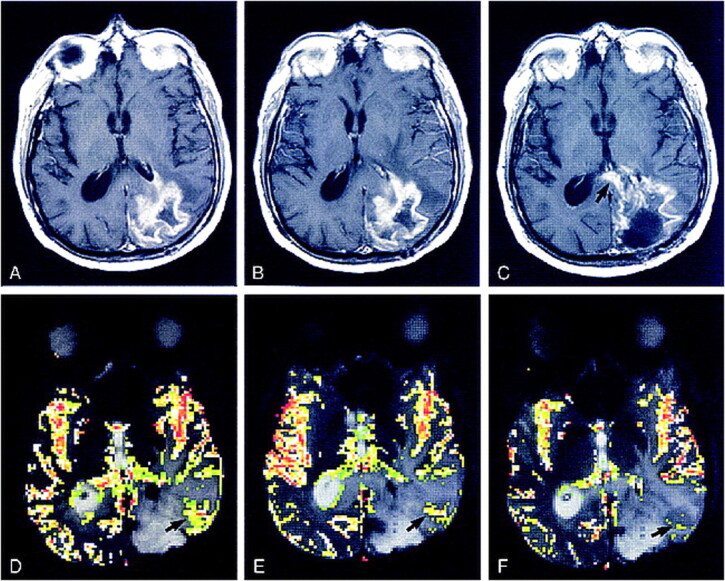
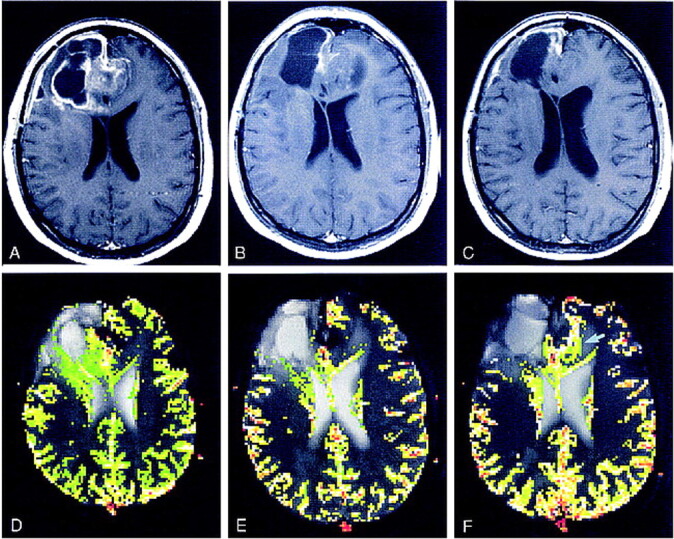
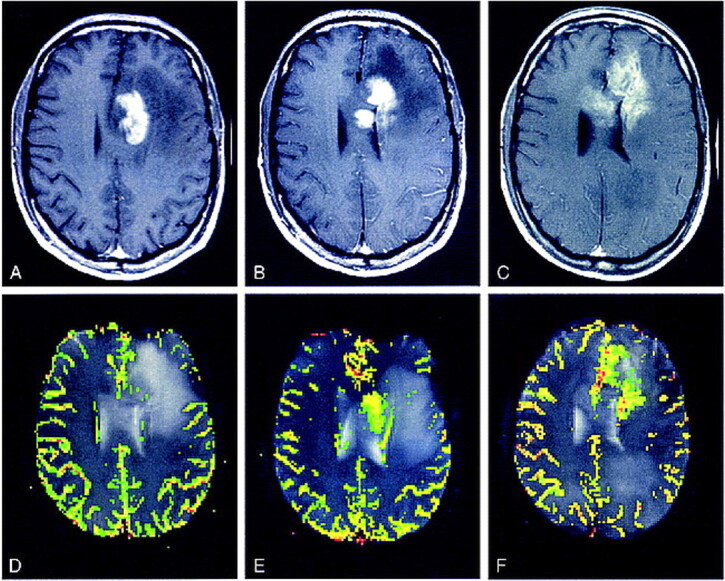
Background and purpose: Dynamic, contrast-enhanced MR imaging has allowed quantitative assessment of cerebral blood volume (CBV) in brain tumors. The purpose of our study was to compare postcontrast T1-weighted imaging with dynamic, contrast-enhanced T2*-weighted echo-planar imaging in the evaluation of the response of recurrent malignant gliomas to thalidomide and carboplatin.
Methods: Serial MR imaging was performed in 18 consecutive patients with recurrent malignant gliomas receiving both thalidomide and carboplatin for 12-month periods. Six patients undergoing carboplatin therapy alone were chosen as control subjects. Conventional postcontrast T1-weighted images were compared with relative CBV (rCBV) maps calculated on a pixel-by-pixel basis from dynamic echo-planar imaging data. Tumor progression was evaluated clinically using established criteria for malignant gliomas. Studies were performed at 2- to 3-month intervals, and imaging and clinical findings were compared.
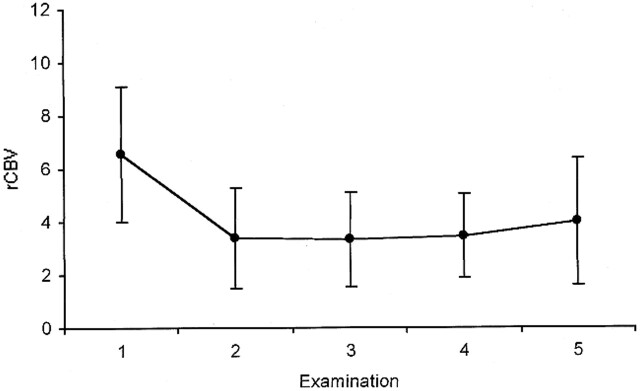
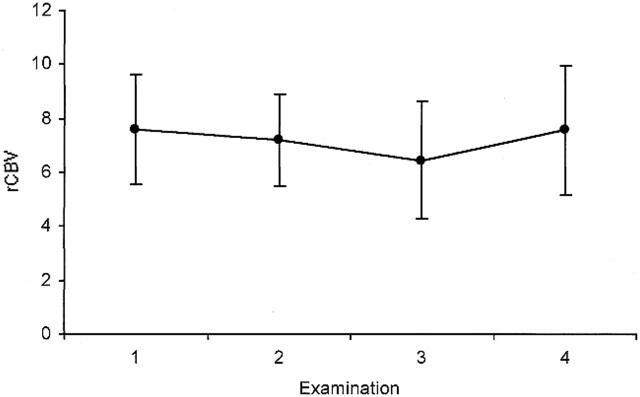
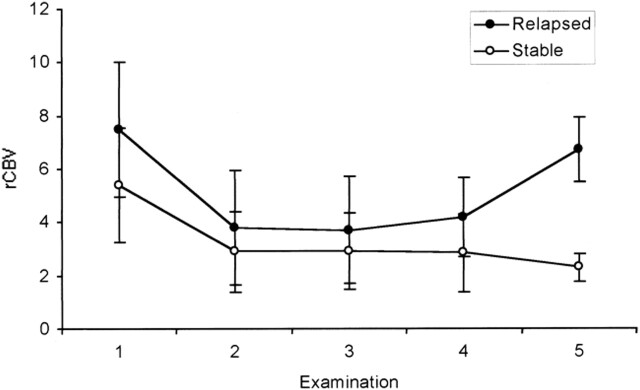
Results: Tumor response to treatment, based on clinical findings, did not correlate well with conventional imaging findings. The rCBV values decreased significantly in all patients between the start of therapy and the first follow-up in the study group, but not in the control group. The difference in rCBV values between the clinically stable and the progressive group at 12-month follow-up was statistically significant, with the progressive group having higher values.
Conclusion: Dynamic, contrast-enhanced MR imaging is a valuable adjunct to conventional imaging in assessing tumor activity during antiangiogenic therapy, and correlates better than conventional studies with clinical status and response to therapy.
Figures
References
-
- Chang SM, Prados MD. Chemotherapy for gliomas. Curr Opin Oncol 1995;7:207-213 - PubMed
-
- Balmaceda C, Fetell MR, Hesdorffer C. Thiotepa and etoposide treatment of recurrent malignant gliomas: phase I study. Cancer Chemother Pharmacol 1997;40:72-74 - PubMed
-
- Friedman HS, Schold SC Jr, Djang WT, et al. Criteria for termination of phase II chemotherapy for patients with progressive or recurrent brain tumor. Neurology 1989;39:62-66 - PubMed
-
- Burger P. Malignant astrocytic neoplasms: classification, pathology, anatomy, and response to therapy. Semin Oncol 1986;13:16-20 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical