

Posttherapeutic intraaxial brain tumor: the value of perfusion-sensitive contrast-enhanced MR imaging for differentiating tumor recurrence from nonneoplastic contrast-enhancing tissue
- PMID: 10815666
- PMCID: PMC7976740
Posttherapeutic intraaxial brain tumor: the value of perfusion-sensitive contrast-enhanced MR imaging for differentiating tumor recurrence from nonneoplastic contrast-enhancing tissue
Abstract
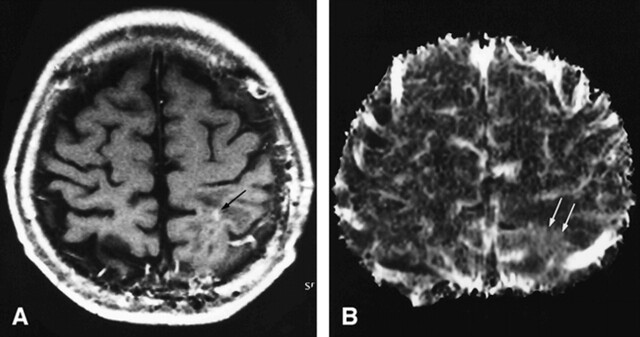
Background and purpose: Differentiation of tumor recurrence from treatment-related changes may be difficult with conventional MR imaging when newly enhancing lesions appear. Our aim was to determine the value of perfusion-sensitive contrast-enhanced MR imaging for differentiating recurrent neoplasm from nonneoplastic contrast-enhancing tissue.
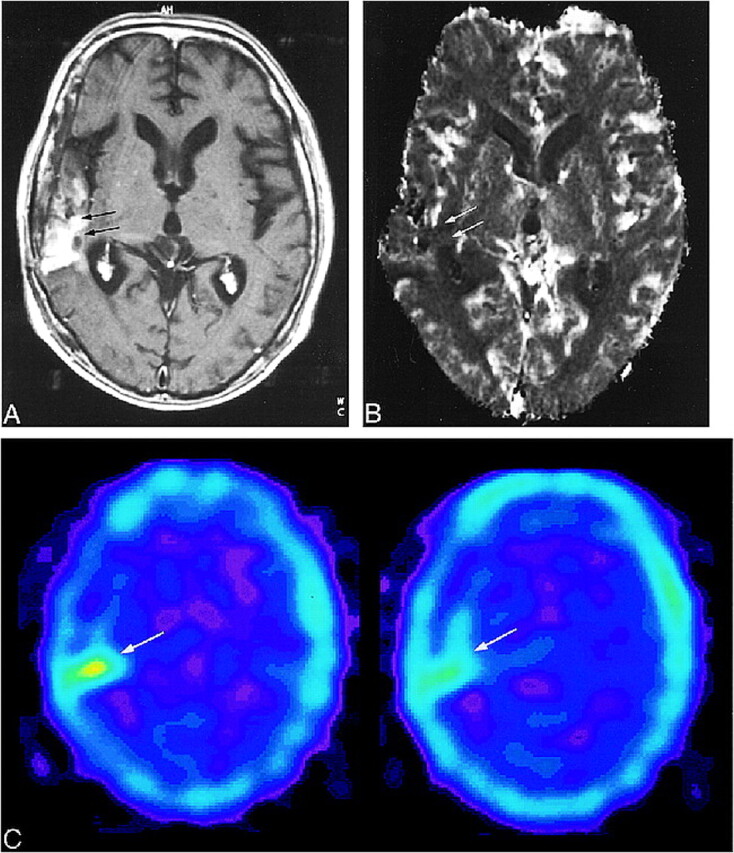
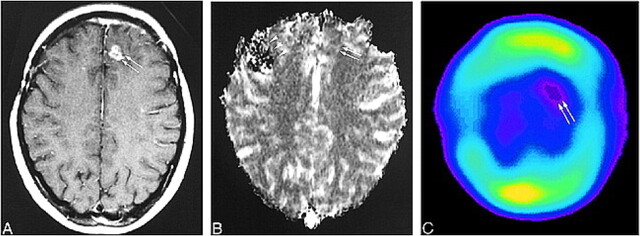
Methods: Twenty patients in whom new enhancing lesions developed within irradiated regions were examined prospectively with perfusion-sensitive contrast-enhanced MR imaging. Twelve of them also underwent thallous chloride Tl 201 single-photon emission tomography (201Tl-SPECT). Normalized relative cerebral blood volume (rCBV) ratios and thallium indexes were evaluated to determine whether the new enhancing lesions were recurrent or not. Five instances of tumor recurrence and one of radiation necrosis were verified histologically; in the others, tumor recurrence was distinguished by lesions that progressively increased in size on serial MR examinations over at least 5 months, and nonneoplastic contrast-enhancing tissue was distinguished by lesions that disappeared or decreased in size on serial MR studies over at least 9 months.
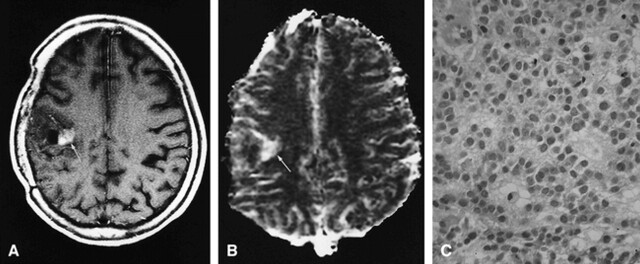
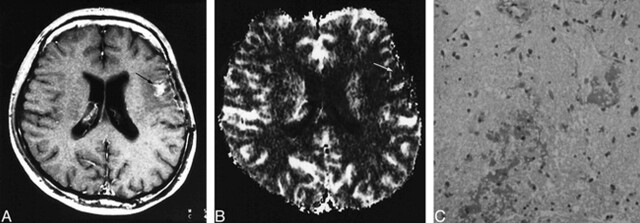
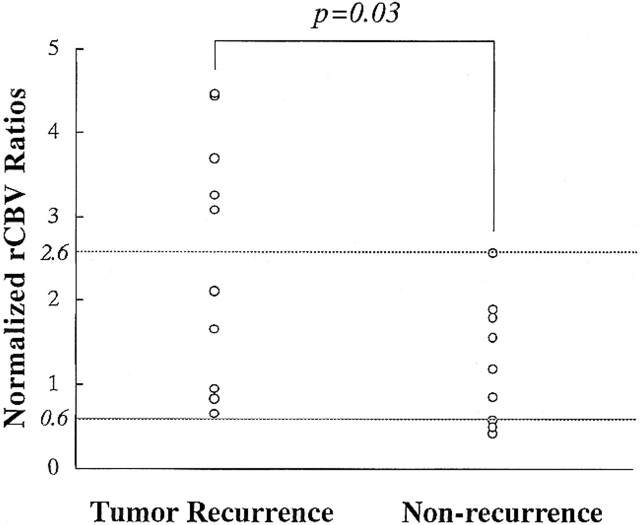
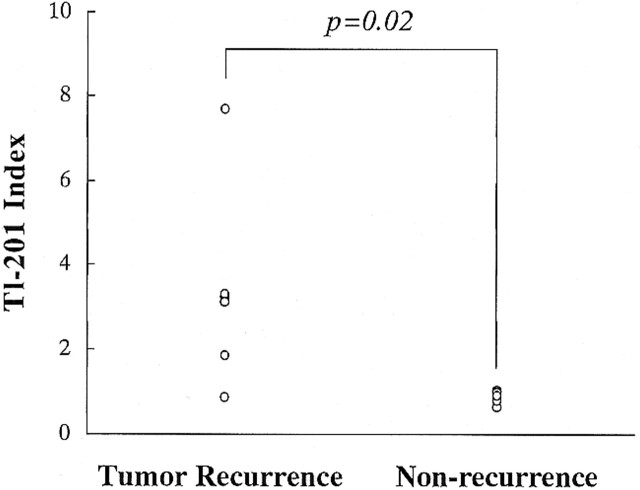
Results: When normalized rCBV ratios were higher than 2.6 or lower than 0.6, enhancing lesions were either recurrent (n = 5) or nonneoplastic contrast-enhancing tissue (n = 3), respectively. All nonneoplastic contrast-enhancing tissue had a low thallium index, whereas three of four recurrent lesions had a high index.
Conclusion: An enhancing lesion with a normalized rCBV ratio higher than 2.6 or lower than 0.6 may suggest tumor recurrence or nonneoplastic contrast-enhancing tissue, respectively. In these cases, further examination with 201Tl-SPECT may not be necessary. However, when the normalized rCBV ratio is between 0.6 and 2.6, 201Tl-SPECT may be useful in making the differentiation.
Figures
References
-
- Tsuruda JS, Kortman KE, Bradley WG, Wheeler DC, Dalsem WV, Bradley TP. Radiation effects on cerebral white matter: MR evaluation. AJR Am J Roentgenol 1987;149:165-171 - PubMed
-
- Remler MP, Marcussen WH, Tiller-Borsich J. The late effects of radiation on the blood brain barrier. Int J Radiat Oncol Biol Phys 1986;12:1965-1969 - PubMed
-
- Dooms GC, Hecht S, Brant-Zawadzki M, Berthiaume Y, Norman D, Newton TH. Brain radiation lesions: MR imaging. Radiology 1986;158:149-155 - PubMed
-
- Nishimura R, Takahashi T, Morishita S, Sumi M, Uozumi H, Sakamoto Y. MR Gd-DTPA enhancement of radiation injury. Radiat Med 1992;10:101-108 - PubMed
-
- Kim EE, Chung SK, Haynie TP, et al. Differentiation of residual or recurrent tumors from post-treatment changes with F-18 FDG PET. Radiographics 1992;12:269-279 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical