

A high-resolution fast spin-echo inversion-recovery sequence for preoperative localization of the internal globus pallidus
- PMID: 10815670
- PMCID: PMC7976753
A high-resolution fast spin-echo inversion-recovery sequence for preoperative localization of the internal globus pallidus
Abstract
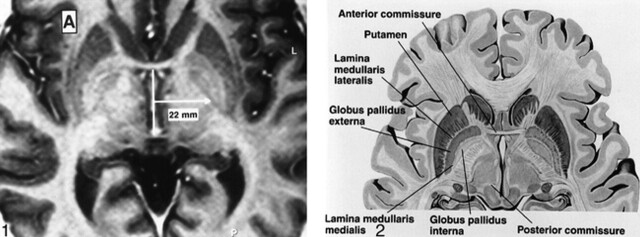
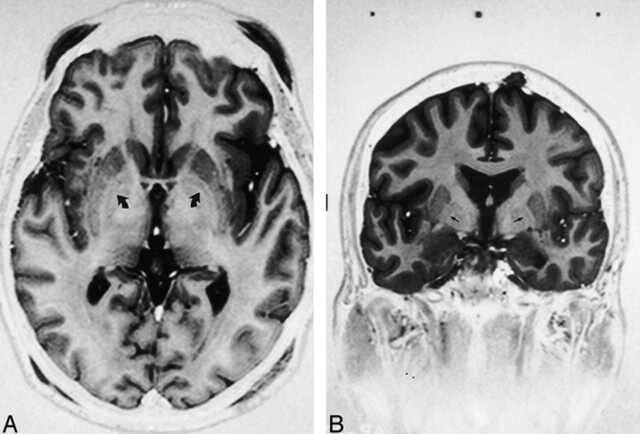
A fast spin-echo inversion-recovery (FSE-IR) sequence is described for its utility regarding surgical planning for patients with Parkinson's disease (PD) who are undergoing microelectrode-guided internal globus pallidus (GPi) ablation. Images from thirty-seven adult patients with PD were reviewed and visualization of the GPi, globus pallidus externa (GPe), and the intervening lamina was noted. High-resolution images were acquired from all patients despite the external hardware and the patients' movement disorder. In all cases, the conventional surgical trajectory, determined indirectly by a fixed measurement from the anteroposterior commissure line, was modified by the ability to visualize the GPi and optic tract directly. This sequence facilitated accurate stereotactic targeting.
Figures
References
-
- Baron MS, Vitek JL, Bakay RA, et al. Treatment of advanced Parkinson's disease by posterior GPi pallidotomy: 1-year results of a pilot study. Ann Neurol 1996;40:355-366 - PubMed
-
- Iacono RP, Shima F, Lonser RR, et al. The results, indications, and physiology of posteroventral pallidotomy for patients with Parkinson's disease. Neurosurgery 1995;36:1128-1127 - PubMed
-
- Laitinen LV, Bergenheim T, Hariz MI. Leksell's posteroventral pallidotomy in the treatment of Parkinson's disease. J Neurosurg 1992;76:53-61 - PubMed
-
- Adams RD, Victor M. Principles of Neurology. 5th ed. New York, NY: McGraw-Hill, Inc 1993 975-982
MeSH terms
LinkOut - more resources
Full Text Sources
Medical