

Choice of surgical technique influences perioperative outcomes in liver transplantation
- PMID: 10816624
- PMCID: PMC1421070
- DOI: 10.1097/00000658-200006000-00005
Choice of surgical technique influences perioperative outcomes in liver transplantation
Abstract
Objective: To examine how the choice of surgical technique influenced perioperative outcomes in liver transplantation.
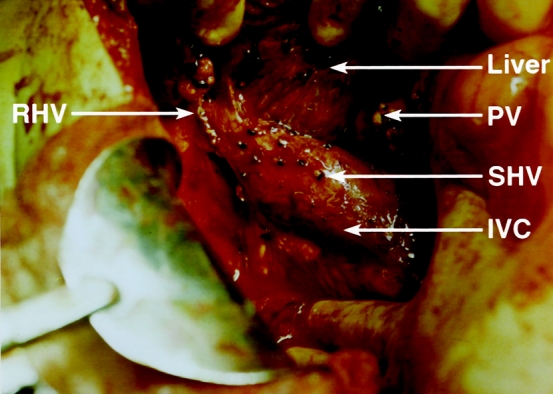
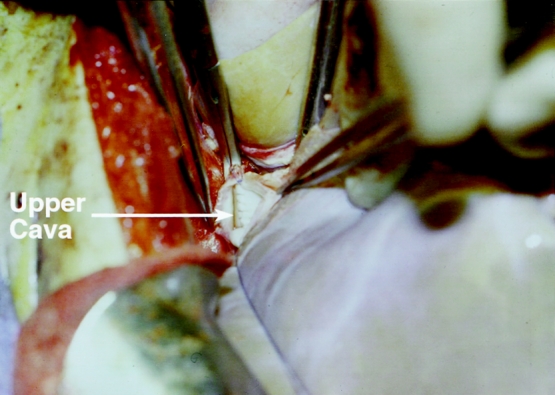
Summary background data: The standard technique of orthotopic liver transplantation with venovenous bypass (VVB) is commonly used to facilitate hemodynamic stability. However, this traditional procedure is associated with unique complications that can be avoided by using the technique of liver resection without caval excision (the piggyback technique).
Methods: A prospective comparison of the two procedures was conducted in 90 patients (34 piggyback and 56 with VVB) during a 2.5-year period. Although both groups had similar donor and recipient demographic characteristics, posttransplant outcomes were significantly better for the patients undergoing the piggyback technique. The effect of surgical technique was examined using a stepwise approach that considered its impact on two levels of perioperative and postoperative events.
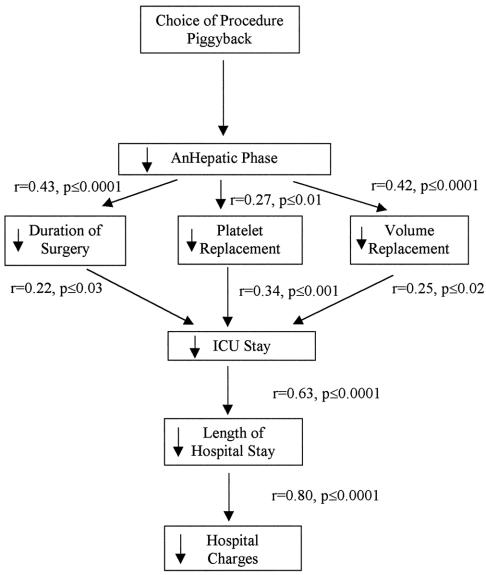
Results: The analysis of the first level of perioperative events found that the piggyback procedure resulted in a 50% decrease in the duration of the anhepatic phase. The analysis of the second level of perioperative events found a significant relation between the anhepatic phase and the duration of surgery and between the anhepatic phase and the need for blood replacement. The analysis of the first level of postoperative events found that the intensive care unit stay was significantly related to both the duration of surgery and the need for blood replacement. The intensive care unit stay was in turn related to the second level of postoperative events, namely the length of hospital stay. Finally, total charges were directly related to length of hospital stay. The overall 1-year actuarial patient and graft survival rates were 94% in the piggyback and 96% in the VVB groups, respectively.
Conclusions: These data demonstrate that surgical choices in complex procedures such as orthotopic liver transplantation trigger a chain of events that can significantly affect resource utilization. In the current healthcare climate, examination of the sequence of events that follow a specific treatment may provide a more complete framework for choosing between treatment alternatives.
Figures
References
-
- Seabert EC, Belle SH, Beringer KC, Schivins JL, Detre KM. Liver transplantation in the United States from 1987–1998: updated results from the Pitt-UNOS Liver Transplant Registry. In: Cecka JM, Terasaki PI, eds. Clinical Transplants 1998. Los Angeles: UCLA Tissue Typing Laboratory; 1998. - PubMed
-
- Paulsen N, Valek TR, Blessing W, et al. Hemodynamics during liver transplantation with veno-venous bypass. Transplant Proc 1987; 21 (1):2417. - PubMed
-
- Khoury G, Martin MD, Mann M, et al. Air embolism associated with veno-venous bypass during orthotopic liver transplantation. Anesthesiology 1987; 67:848. - PubMed
-
- Navalgund A, Kang Y, Sarner J, Jahr J, Gieraerts R. Massive pulmonary thromboembolism during liver transplantation. Anesth Analg 1988; 67:400. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
