

The impact of patients' preferences on the treatment of atrial fibrillation: observational study of patient based decision analysis
- PMID: 10818030
- PMCID: PMC27382
- DOI: 10.1136/bmj.320.7246.1380
The impact of patients' preferences on the treatment of atrial fibrillation: observational study of patient based decision analysis
Abstract
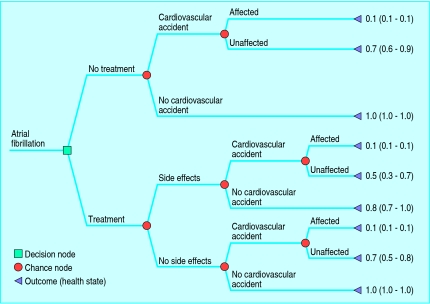
Objective: To investigate the impact of patients' preferences for the treatment of atrial fibrillation, by using individualised decision analysis combining probability and utility assessments into a decision tree.
Design: Observational study based on interviews with patients.
Setting: Eight general practices in Avon.
Participants: 260 randomly selected patients aged 70-85 years with atrial fibrillation.
Main outcome measures: Patients' treatment preferences regarding anticoagulation treatment (warfarin) after individualised decision analysis; comparison of these preferences with treatment guidelines on the basis of comorbidity and absolute risk and compared with current prescription.
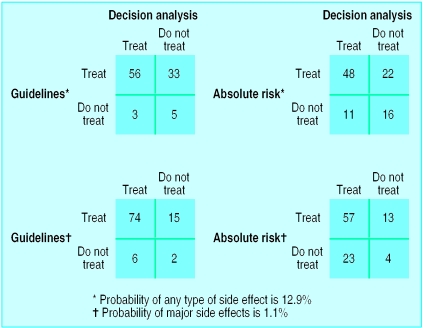
Results: Of 195 eligible patients, 97 participated in decision making using decision analysis. Among these 97, the decision analysis indicated that 59 (61%; 95% confidence interval 50% to 71%) would prefer anticoagulation treatment-considerably fewer than those who would be recommended treatment according to guidelines. There was marked disagreement between the decision analysis and guideline recommendations (kappa=0.25 or less). Of 38 patients whose decision analysis indicated a preference for anticoagulation, 17 (45%) were being prescribed warfarin; on the other hand, 28 (47%) of 59 patients were not being prescribed warfarin although the results of their decision analysis suggested they wanted to be.
Conclusions: In the context of shared decision making, individualised decision analysis is valuable in a sizeable proportion of elderly patients with atrial fibrillation. Taking account of patients' preferences would lead to fewer prescriptions for warfarin than under published guideline recommendations. Decision analysis as a shared decision making tool should be evaluated in a randomised controlled trial.
Figures
Comment in
-
Commentary: patients, preferences, and evidence.BMJ. 2000 May 20;320(7246):1384. BMJ. 2000. PMID: 10858048 No abstract available.
References
-
- Atrial Fibrillation Investigators. Risk factors for stroke and efficacy of antithrombotic therapy in atrial fibrillation. Arch Intern Med. 1994;154:1449–1457. - PubMed
-
- Sudlow M, Thomson R, Thwaites B, Rodgers H, Kenny RA. Prevalence of atrial fibrillation and eligibility for anticoagulants in the community. Lancet. 1998;352:1167–1171. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical