

A clinical pathway to accelerate recovery after colonic resection
- PMID: 10862195
- PMCID: PMC1421107
- DOI: 10.1097/00000658-200007000-00008
A clinical pathway to accelerate recovery after colonic resection
Abstract
Objective: To investigate the feasibility of a 48-hour postoperative stay program after colonic resection.
Summary background data: Postoperative hospital stay after colonic resection is usually 6 to 12 days, with a complication rate of 10% to 20%. Limiting factors for early recovery include stress-induced organ dysfunction, paralytic ileus, pain, and fatigue. It has been hypothesized that an accelerated multimodal rehabilitation program with optimal pain relief, stress reduction with regional anesthesia, early enteral nutrition, and early mobilization may enhance recovery and reduce the complication rate.
Methods: Sixty consecutive patients undergoing elective colonic resection were prospectively studied using a well-defined postoperative care program including continuous thoracic epidural analgesia and enforced early mobilization and enteral nutrition, and a planned 48-hour postoperative hospital stay. Postoperative follow-up was scheduled at 8 and 30 days.
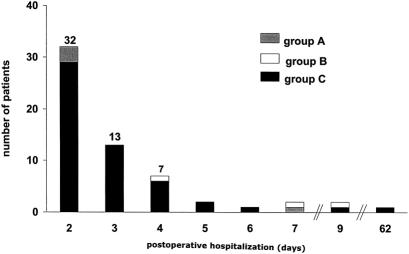
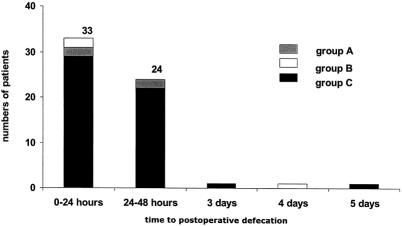
Results: Median age was 74 years, with 20 patients in ASA group III-IV. Normal gastrointestinal function (defecation) occurred within 48 hours in 57 patients, and the median hospital stay was 2 days, with 32 patients staying 2 days after surgery. There were no cardiopulmonary complications. The readmission rate was 15%, including two patients with anastomotic dehiscence (one treated conservatively, one with colostomy); other readmissions required only short-term observation.
Conclusion: A multimodal rehabilitation program may significantly reduce the postoperative hospital stay in high-risk patients undergoing colonic resection. Such a program may also reduce postoperative ileus and cardiopulmonary complications. These results may have important implications for the care of patients after colonic surgery and in the future assessment of open versus laparoscopic colonic resection.
Figures
References
-
- Retchen SM, Penberthy L, Desch C, et al. Perioperative management of colonic cancer under Medicare risk programs. Arch Intern Med 1997; 157:1878–1884. - PubMed
-
- Schoetz DJ, Bockler M, Rosenblat MS, et al. “Ideal” length of stay after colectomy: whose ideal? Dis Colon Rectum 1997; 40:806–810. - PubMed
-
- Bokey EL, Chapuis PH, Fung C, et al. Postoperative morbidity and mortality following resection of the colon and rectum cancer. Dis Colon Rectum 1995; 38:480–487. - PubMed
-
- Marcario A, Vitez TS, Dunn B, et al. Hospital costs and severity of illness in three types of elective surgery. Anesthesiology 1997; 86:92–100. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
