

Chronic liver allograft rejection in a population treated primarily with tacrolimus as baseline immunosuppression: long-term follow-up and evaluation of features for histopathological staging
- PMID: 10868635
- PMCID: PMC2967190
- DOI: 10.1097/00007890-200006150-00019
Chronic liver allograft rejection in a population treated primarily with tacrolimus as baseline immunosuppression: long-term follow-up and evaluation of features for histopathological staging
Abstract
Background: Predisposing factors, long-term occurrence, and histopathological changes associated with recovery or progression to allograft failure from chronic rejection (CR) were studied in adult patients treated primarily with tacrolimus.
Methods: CR cases were identified using stringent criteria applied to a retrospective review of computerized clinicopathological data and slides.
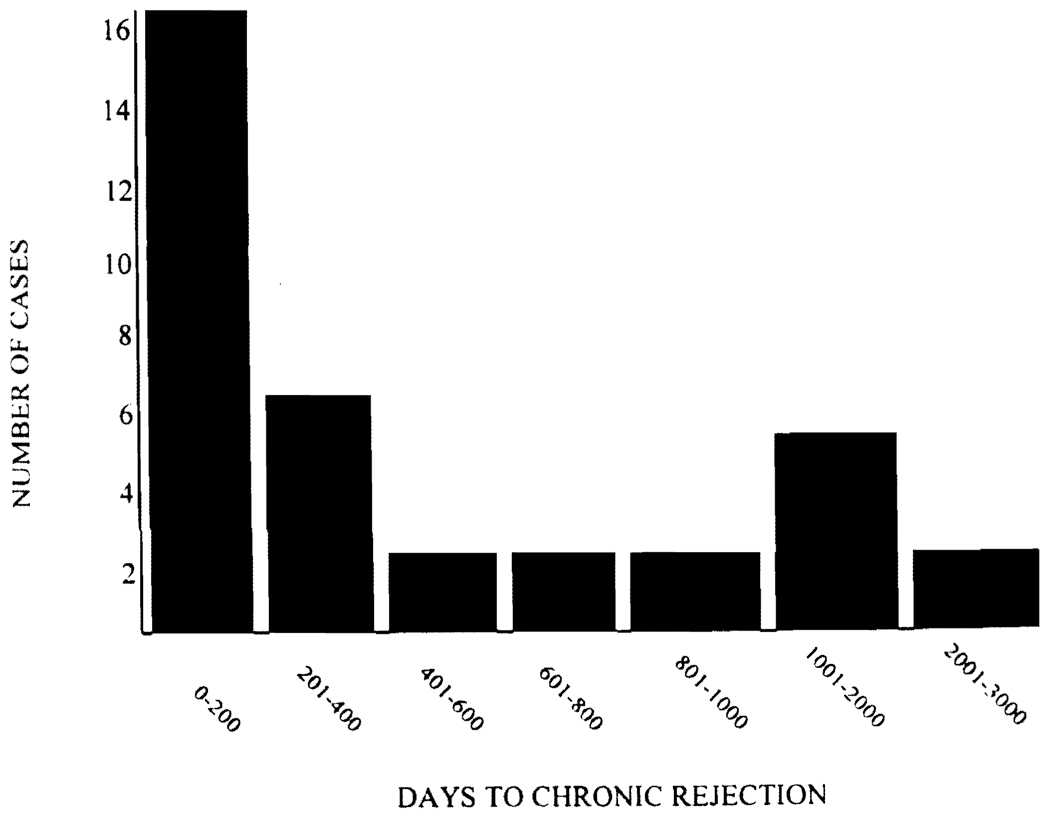
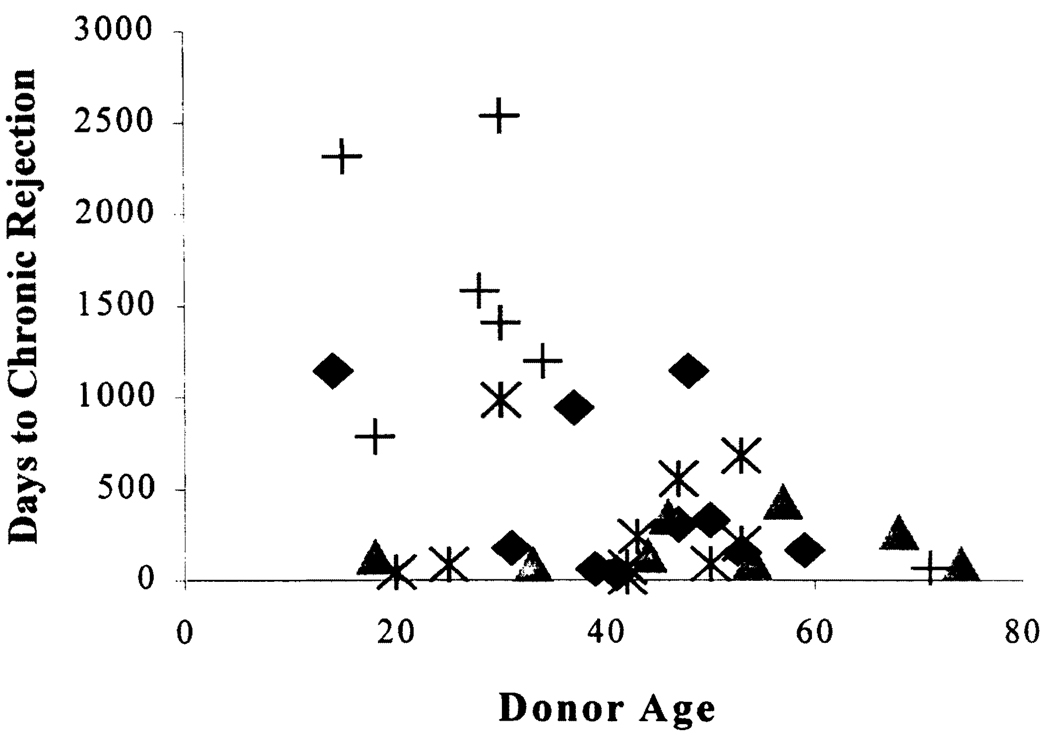
Results: After 1973 days median follow-up, 35 (3.3%) of 1049 primary liver allograft recipients first developed CR between 16 and 2532 (median 242) days. The most significant risk factors for CR were the number (P<0.001) and histological severity (P<0.005) of acute rejection episodes and donor age >40 years (P<0.03). Other demographic and matching parameters were not associated with CR in this cohort. Ten patients died with, but not of, CR. Eight required retransplantation because of CR at a median of 268 days. Ten resolved either histologically or by normalization of liver injury tests over a median of 548 days. CR persisted for 340 to 2116 days in the remaining seven patients. More extensive bile duct loss (P<0.01), smallarterial loss (P<0.03), foam cell clusters (P<0.01) and higher total bilirubin (P<0.02) and aspartate aminotransferase (P<0.03) were associated with allograft failure from CR.
Conclusions: Early chronic liver allograft rejection is potentially reversible and a combination of histological, clinical, and laboratory data can be used to stage CR. Unique immunological and regenerative properties of liver allografts, which lead to a low incidence and reversibility of early CR, can provide insights into transplantation biology.
Figures
References
-
- Pirsch JD, Kalayoglu M, Hafez GR, D’Alessandro AM, Sollinger HW, Belzer FD. Evidence that the vanishing bile duct syndrome is vanishing. Transplantation. 1990;49(5):1015. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
