

Cranial MR imaging of osteopetrosis
Abstract
Background and purpose: The purpose of this study was to describe the cranial MR imaging manifestations of osteopetrosis. These features have not previously been reported in the literature.
Methods: Cranial MR studies, obtained with a uniform imaging protocol, were reviewed in 47 patients with osteopetrosis. Thirty-four patients had autosomal recessive (malignant) osteopetrosis (AROP), seven had intermediate osteopetrosis (IOP), and six had either type I or type II autosomal dominant osteopetrosis (ADOP I or II). The prevalence of abnormalities was tabulated and compared with the specific osteopetrosis variants.
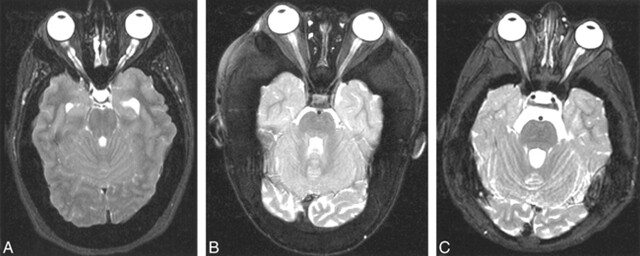
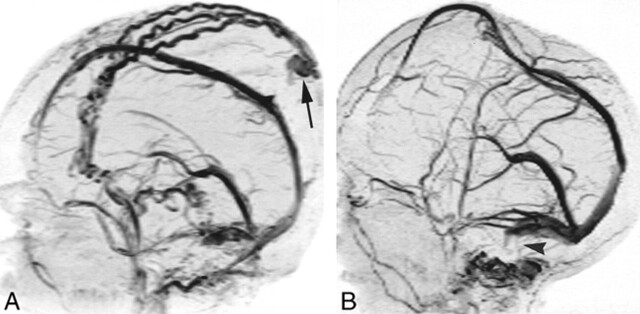
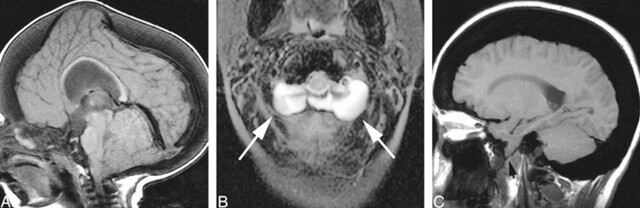
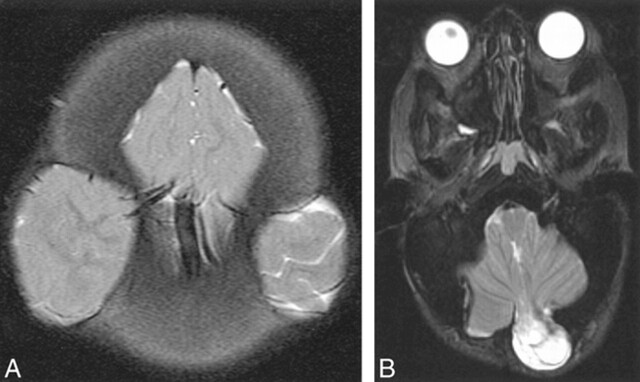
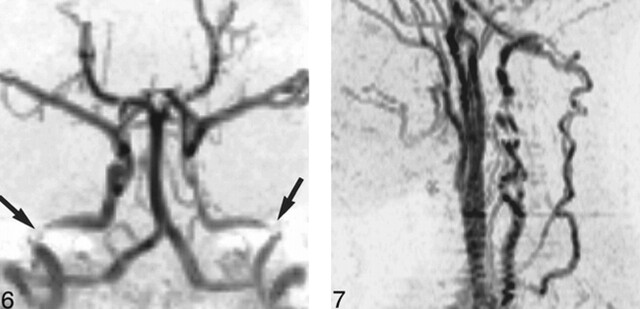
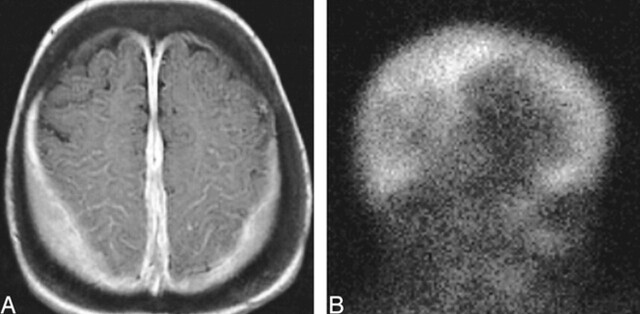
Results: All patients with osteopetrosis had thickening and sclerosis of the calvaria. Ventriculomegaly, tonsillar herniation, proptosis, and dural venous sinus stenosis were observed in the majority of patients with AROP and ADOP I. Optic nerve sheath dilatation occurred in many of the patients with AROP and in all patients with ADOP I. Acquired cephaloceles were also observed only in these two groups. Optic nerve atrophy and optic canal stenosis were observed in a majority of patients with AROP, IOP, and ADOP II. Middle ear fluid was prevalent in AROP and IOP, present in over half the patients in each group. Features seen most prevalently, or exclusively, in AROP included stenosis of the internal carotid and vertebral arteries and extramedullary hematopoiesis.
Conclusion: The cranial MR imaging features of osteopetrosis are both shared and unique among the various subtypes of the disease. The specific cranial and intracranial manifestations reflect the predominant calvarial or skull base patterns of bone thickening. The unique features seen in patients with AROP probably reflect the early age of onset and the greater severity of this form of the disease.
Figures

References
-
- Whyte MP. Sclerosing bone dysplasias. In: Favus MJ, ed. Primer on the Metabolic Bone Diseases and Disorders of Mineral Metabolism. 2nd ed. New York: Raven; 1993 327-330
-
- Makin GJV, Coates RK, Pelz D, et al. Major cerebral arterial and venous disease in osteopetrosis. Stroke 1986;17:106-110 - PubMed
-
- Wilms G, Casaer P, Alliet P, et al. Cerebrovascular occlusive complications in osteopetrosis major. Neuroradiology 1990;32:511-513 - PubMed
-
- Curé JK, Key LL, Shankar L, Gross AJ. Petrous carotid canal stenosis in malignant osteopetrosis: CT documentation with MR angiographic correlation. Radiology 1996;199:415-421 - PubMed
-
- Kahler SG, Burns JA, Ayslworth AS. A mild autosomal recessive form of osteopetrosis. Am J Med Gen 1984;17:451-464 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical