

Review
Diffuse leptomeningeal oligodendrogliomatosis: radiologic/pathologic correlation
Affiliations
- PMID: 10871026
- PMCID: PMC7973905
Item in Clipboard
Review
Diffuse leptomeningeal oligodendrogliomatosis: radiologic/pathologic correlation
AJNR Am J Neuroradiol.
2000 Jun-Jul.
Abstract
We present the radiologic and pathologic findings in a boy who presented with diffuse leptomeningeal enhancement and whose clinical status deteriorated over the course of 5 years. During this period, MR images showed progression of the enhancement in the subarachnoid spaces, formation of intraaxial cysts, and hydrocephalus. Autopsy findings revealed diffuse oligodendroglioma throughout the leptomeninges of the brain and spine, with no definite intraaxial focus. The radiologic and pathologic features of diffuse leptomeningeal oligodendrogliomatosis are reviewed.
Figures
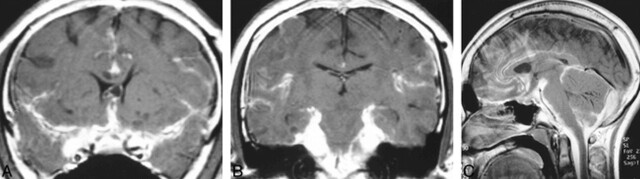
MR images obtained at initial presentation. A, Coronal contrast-enhanced T1-weighted image shows diffuse enhancement of the subarachnoid space at the level of the suprasellar and sylvian fissure cisterns and along the interhemispheric fissure. There is no hydrocephalus, although there is questionable expansion of the cavum septum pellucidi. Small cystlike lesions are present in the left basal ganglia. B, Coronal contrast-enhanced T1-weighted image posterior to A shows marked enhancement surrounding the brain stem. C, Midsagittal contrast-enhanced T1-weighted image shows enhancement of the CSF-containing spaces, particularly at the base of the skull.
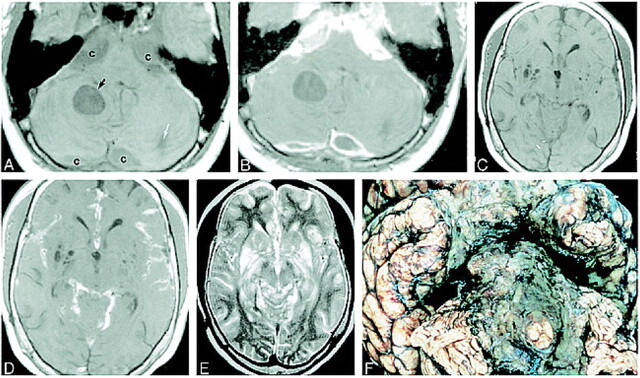
MR images obtained 1 month before death of patient and gross pathologic correlation. A, Axial noncontrast T1-weighted image shows expansion of the cisterns (c), which are slightly inhomogeneous in appearance and of higher signal intensity than expected for normal CSF. There is a well-defined intraaxial cyst (black arrow) and a smaller one (white arrow) in the posterior left cerebellar hemisphere. B, Corresponding contrast-enhanced T1-weighted image shows marked enhancement of the extraaxial abnormalities surrounding the brain stem. The cysts in the region of the cisterna magna show peripheral enhancement. The intraaxial cysts do not enhance. C, Noncontrast axial T1-weighted image shows multiple cystlike lesions in the basal ganglia bilaterally. D, Corresponding contrast-enhanced T1-weighted image shows enhancement of subarachnoid spaces in sylvian fissures and quadrigeminal plate and superior cerebellar cisterns. The lesions in the basal ganglia do not enhance. All lesions were hyperintense on T2-weighted images. E, Axial T2-weighted image corresponding to C and D shows that the lesions in the cisterns, cortical sulci, and dilated perivascular spaces in the region of the basal ganglia are of high signal intensity. F, Basal view of fixed brain shows thickened opaque leptomeninges encasing the brain stem and basal cisterns. These leptomeninges are diffusely infiltrated by tumor.
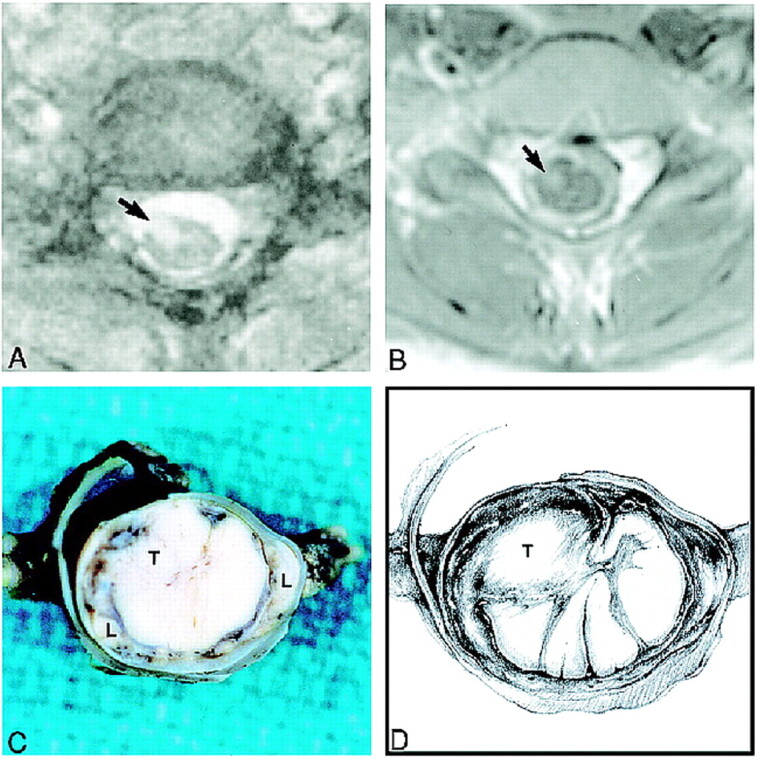
Spine MR images obtained during the last admission and gross pathologic correlation. A, Axial T2-weighted image at the C6–C7 level shows an intramedullary spinal cord lesion (arrow). The subarachnoid spaces appear widened. B, Corresponding contrast-enhanced T1-weighted image shows that the spinal cord lesion (arrow) enhances. The spinal cord appears hypointense and is surrounded by thick and enhancing subarachnoid space. C, Fixed gross specimen shows a relatively well-circumscribed intramedullary tumor (T) within the cervical spinal cord surrounded by a dense cuff of leptomeninges (L). D, Drawing depicts location of tumor nodule (T) and tumor infiltrating the leptomeninges.
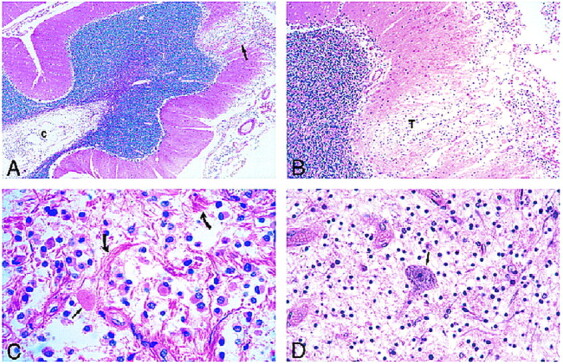
Photomicrographs of sections stained with hematoxylin-eosin. A, Low-power view of the cerebellum shows leptomeningeal infiltrate and superficial cortical tumor invasion (arrow) with cystic rarefaction (c) of deep white matter by tumor. B, Medium-power view of area of cortical tumor invasion shown in A reveals neoplastic cells (T) in a rarefied area of cortex. C, The leptomeningeal infiltrate is composed of a monomorphous population of noncohesive cells with interspersed eosinophilic granular bodies (straight arrow) and marked fibrous proliferation (curved arrows). D, View of spinal cord lesion shows an isolated anterior horn neuron (arrow) in a background of tumor cells.
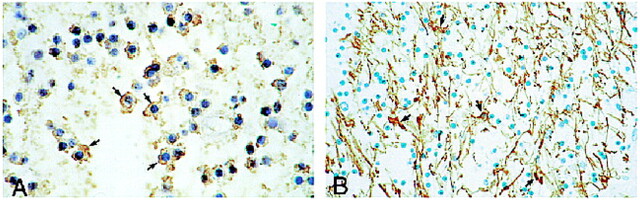
Immunocytochemistry. A, High-power view shows positive immunoreactivity of neoplastic cells for Leu 7 (CD57). Note dark brown cytoplasmic immunostaining (arrows) of neoplastic oligodendrocytes. B, Medium-power view shows a negative immunoreactivity of neoplastic cells for GFAP. Residual reactive astrocytes stain positively (arrows) whereas neoplastic cells are devoid of positive staining.
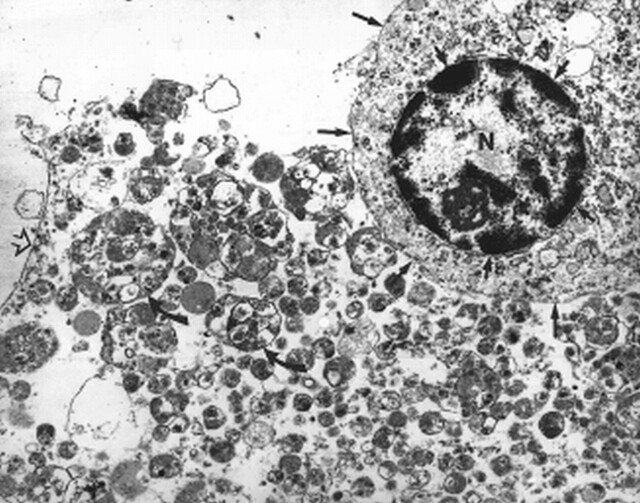
Electron microscopic view shows one tumor cell with a round regular nucleus (N), peripherally clumped chromatin (short arrows), and surrounding small amount of cytoplasm (long arrows point to cytoplasmic membrane). Adjacent to the tumor cell are numerous extracellular lysosomes (curved arrows) and a fragmented cell membrane (open arrow)
References
-
- Beck DJK, Russell DS. Oligodendrogliomatosis of the cerebrospinal fluid pathway. Brain 1942;65:352-372
-
- Perentes E, Rubinstein LJ. Recent applications of immunoperoxidase histochemistry in human neuro-oncology. Arch Pathol Lab Med 1989;111:796-812 - PubMed
-
- Russell DS. Observations on the pathology of hydrocephalus. In: Medical Research Council, Special Report, Series No. 265. London: His Majesty's Stationary Office; 1949 112-113
-
- Michel D, Lemercier G, Beau G, Tommasi M, Schott B. Gliomatose méningée et ventriculaire diffuse secondaire à un oligodendrogliome intramédullaire: a propos d'une observation. Lyon Med 1975;234:37-41
-
- Toso V. Diffusioni metastiche alle leptomeningi. Acta Neurol Napoli 1967;22:366-376 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources