

Recurrent genetic aberrations in thymoma and thymic carcinoma
- PMID: 10880395
- PMCID: PMC1850202
- DOI: 10.1016/S0002-9440(10)64536-1
Recurrent genetic aberrations in thymoma and thymic carcinoma
Abstract
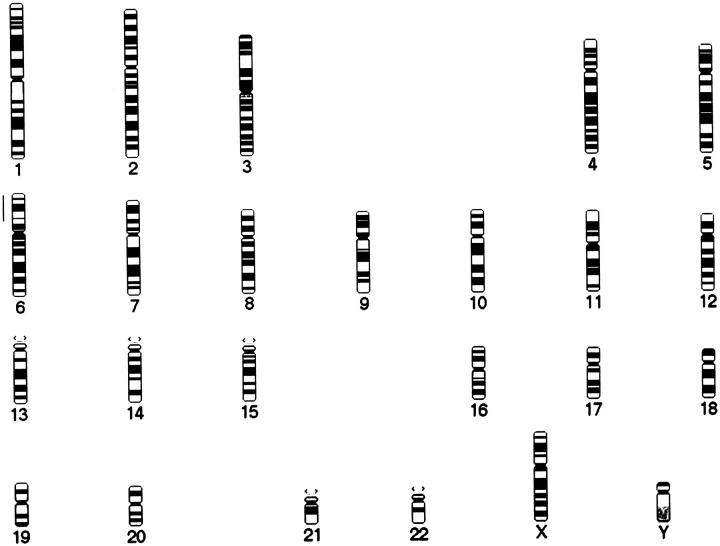
Apart from single reported aberrant karyotypes, genetic alterations in thymic epithelial neoplasms have not been investigated so far. In this study, 12 World Health Organization classification type A thymomas (medullary thymomas), 16 type B3 thymomas (well-differentiated thymic carcinomas), and nine type C thymomas, all of them primary thymic squamous cell carcinomas, were analyzed by comparative genomic hybridization and fluorescence in situ hybridization. With the exception of one single case, type A thymomas did not reveal chromosomal gains or losses in comparative genomic hybridization. In contrast, all type B3 thymomas showed chromosomal imbalances, with gain of 1q, loss of chromosome 6, and loss of 13q occurring in 11 (69%), six (38%), and five (31%) of 16 cases, respectively. In primary thymic squamous cell carcinoma, the most frequent chromosomal losses were observed for 16q (six of nine cases, 67%), 6 (4 of 9, 44%), and 3p and 17p (three of nine each, 33%), whereas recurrent gains of chromosomal material were gains of 1q (5 of 9, 56%), 17q, and 18 (three of nine each, 33%). This study shows that the distinct histological thymoma types A and B3 exhibit distinct genetic phenotypes, whereas type B3 thymoma and primary thymic squamous cell carcinoma partially share genetic aberrations. In addition to the possible tumorigenic role, the deletion in type B3 thymoma of chromosome 6, harboring the HLA locus, might play a role in the pathogenesis of paraneoplastic autoimmunity characteristic of thymoma.
Figures



References
-
- Rosai J, Sobin LH: Histological typing of tumours of the thymus. World Health Organization International Histological Classification of Tumours. 1999, :pp 1-65 Springer Verlag, Heidelberg
-
- Levine GD, Rosai J: Thymic hyperplasia and neoplasia. A review of current concepts. Hum Pathol 1978, 9:495-515 - PubMed
-
- Lewis JE, Wick MR, Scheithauer BW, Bernatz PE, Taylor WF: Thymoma: a clinicopathologic review. Cancer 1987, 60:2727-2743 - PubMed
-
- Quintanilla-Martinez L, Wilkins EW, Ferry JA, Harris NL: Thymoma: morphologic subclassification correlates with invasiveness and immunohistologic features. A study of 122 cases. Hum Pathol 1993, 24:958-969 - PubMed
-
- Quintanilla-Martinez L, Wilins EW, Choi N, Efrid J, Hug E, Harris NL: Thymoma: histologic subclassification is an independent prognostic factor. Cancer 1994, 74:606-617 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
