

Percutaneous transluminal coronary angioplasty versus medical treatment for non-acute coronary heart disease: meta-analysis of randomised controlled trials
- PMID: 10884254
- PMCID: PMC27425
- DOI: 10.1136/bmj.321.7253.73
Percutaneous transluminal coronary angioplasty versus medical treatment for non-acute coronary heart disease: meta-analysis of randomised controlled trials
Abstract
Objective: To determine whether percutaneous transluminal coronary angioplasty (angioplasty) is superior to medical treatment in non-acute coronary artery disease.
Design: Meta-analysis of randomised controlled trials.
Setting: Randomised controlled trials conducted worldwide and published between 1979 and 1998.
Participants: 953 patients treated with angioplasty and 951 with medical treatment from six randomised controlled trials, three of which included patients with multivessel disease and pre-existing myocardial infarction.
Main outcome measures: Angina, fatal and non-fatal myocardial infarction, death, repeated angioplasty, and coronary artery bypass grafting.
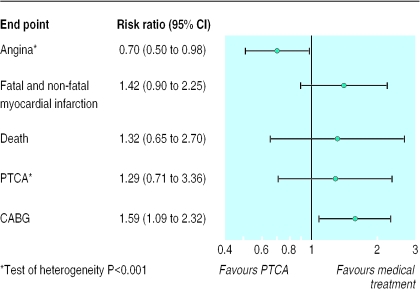
Results: In patients treated with angioplasty compared with medical treatment the risk ratios were 0. 70 (95% confidence interval 0.50 to 0.98; heterogeneity P<0.001) for angina; 1.42 (0.90 to 2.25) for fatal and non-fatal myocardial infarction, 1.32 (0.65 to 2.70) for death, 1.59 (1.09 to 2.32) for coronary artery bypass graft, and 1.29 (0.71 to 3.36; heterogeneity P<0.001) for repeated angioplasty. Differences in the methodological quality of the trials, in follow up, or in single versus multivessel disease did not explain the variability in study results in any analysis.
Conclusions: Percutaneous transluminal coronary angioplasty may lead to a greater reduction in angina in patients with coronary heart disease than medical treatment but at the cost of more coronary artery bypass grafting. Trials have not included enough patients for informative estimates of the effect of angioplasty on myocardial infarction, death, or subsequent revascularisation, though trends so far do not favour angioplasty.
Figures
Comment in
- ACP J Club. 2001 Jan-Feb;134(1):4
-
Treatment of stable angina. Use drugs before percutaneous transluminal coronary angioplasty.BMJ. 2000 Jul 8;321(7253):62-3. doi: 10.1136/bmj.321.7253.62. BMJ. 2000. PMID: 10884235 Free PMC article. No abstract available.
-
Studies in meta-analysis of treatment of stable angina had methodological flaws.BMJ. 2000 Dec 2;321(7273):1408. BMJ. 2000. PMID: 11099295 Free PMC article. No abstract available.
References
-
- Gillum BS, Graves EJ, Kozak KJ National Center for Health Statistics. Trends in hospital utilization: United States, 1988-92. Washington, DC: Government Printing Office; 1996. . (DHHS publication No (PHS) 96-1785. Series 13. No 124.) - PubMed
-
- Higginson LA, Cairns JA, Smith ER. Rates of cardiac catheterization, coronary angioplasty and coronary artery bypass surgery in Canada (1991) Can J Cardiol. 1994;10:728–732. - PubMed
-
- Weaver WD, Simes RJ, Betriu A, Grines CL, Zijlstra F, Garcia E, et al. Comparison of primary coronary angioplasty and intravenous thrombolytic therapy for acute myocardial infarction: a quantitative review. JAMA. 1997;278:2093–2098. - PubMed
-
- Michels KB, Yusuf S. Does PTCA in acute myocardial infarction affect mortality and reinfarction rates? A quantitative overview (meta-analysis) of the randomized clinical trials. Circulation. 1995;91:476–485. - PubMed
-
- Bates DW, Miller E, Bernstein SJ, Hauptman PJ, Leape LL. Coronary angiography and angioplasty after acute myocardial infarction. Ann Intern Med. 1997;126:539–550. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical