

Mapping of a gene for severe pediatric gastroesophageal reflux to chromosome 13q14
- PMID: 10891964
- PMCID: PMC6148744
- DOI: 10.1001/jama.284.3.325
Mapping of a gene for severe pediatric gastroesophageal reflux to chromosome 13q14
Abstract
Context: Gastroesophageal reflux (GER) has not previously been widely regarded as a hereditary disease. A few reports have suggested, however, that a genetic component may contribute to the incidence of GER, especially in its severe or chronic forms.
Objective: To identify a genetic locus that cosegregates with a severe pediatric GER phenotype in families with multiple affected members.
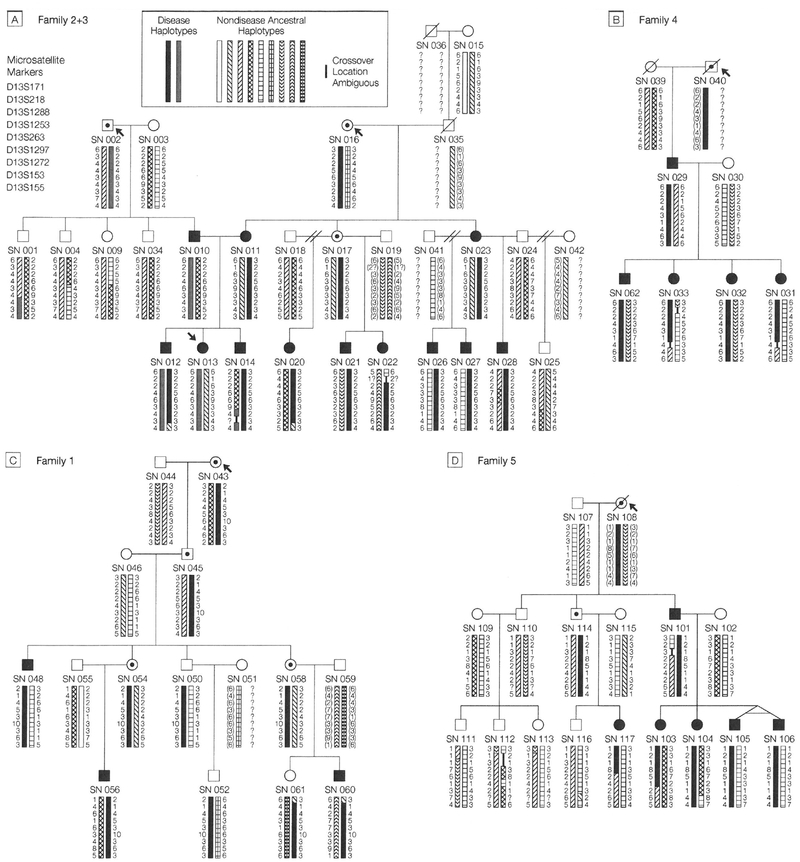
Design: A genome-wide scan of families affected by severe pediatric GER using polymorphic microsatellite markers spaced at an average of 8 centimorgans (cM), followed by haplotyping and by pairwise and multipoint linkage analyses.
Setting: General US community, with research performed in a university tertiary care hospital.
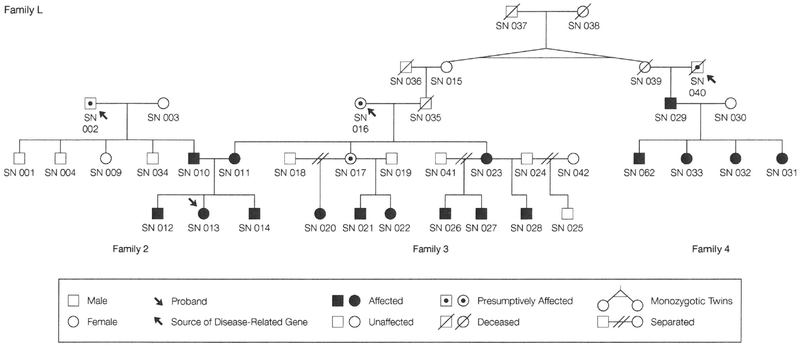
Subjects: Affected and unaffected family members from 5 families having multiple individuals affected by severe pediatric GER, identified through a patient support group.
Main outcome measures: Determination of inheritance patterns and linkage of a genetic locus with the severe pediatric GER phenotype by logarithm-of-odds (lod) score analysis, considering a lod score of 3 or greater as evidence of linkage.
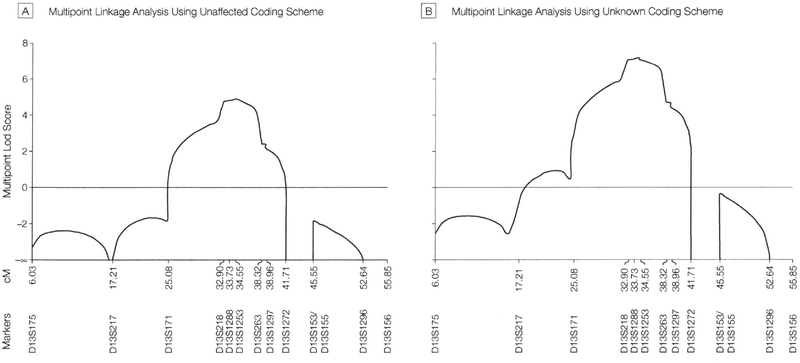
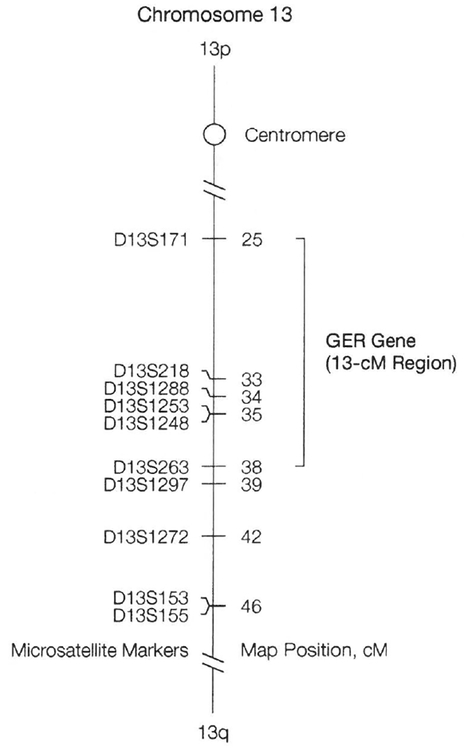
Results: In these families, severe pediatric GER followed an autosomal dominant hereditary pattern with high penetrance. A gene for severe pediatric GER was mapped to a 13-cM region on chromosome 13q between microsatellite markers D13S171 and D13S263. A maximum multifamily 2-point lod score of 5.58 and a maximum multifamily multipoint lod score of 7.15 were obtained for marker D13S1253 at map position 35 cM when presumptively affected persons were modeled as unknown (a maximum multipoint score of 4.88 was obtained when presumptively affected persons were modeled as unaffected).
Conclusion: These data suggest that a gene for severe pediatric GER maps to chromosome 13q14. JAMA. 2000;284:325-334
Figures
Comment in
-
The spectrum of pediatric gastroesophageal reflux.JAMA. 2000 Dec 27;284(24):3125-6. doi: 10.1001/jama.284.24.3125. JAMA. 2000. PMID: 11135768 No abstract available.
References
-
- Fonkalsrud EW, Ament ME. Gastroesophageal reflux in childhood. Curr Probl Surg. 1996;33:1–70. - PubMed
-
- Romero Y, Locke GR III. Is there a GERD gene? Am J Gastroenterol. 1999;94:1127–1129. - PubMed
-
- Lagergren J, Bergstrom R, Lindgren A, Nyren O. Symptomatic gastroesophageal reflux as a risk factor for esophageal adenocarcinoma. N Engl J Med. 1999; 340:825–831. - PubMed
-
- Euler AR. Upper respiratory tract complications of gastroesophageal reflux in adult and pediatric-age patients. Dig Dis. 1998;16:111–117. - PubMed
-
- McMurray JS, Holinger LD. Otolaryngic manifestations in children presenting with apparent life-threatening events. Otolaryngol Head Neck Surg. 1997; 116:575–579. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
