

Immunologic self-tolerance maintained by CD25(+)CD4(+) regulatory T cells constitutively expressing cytotoxic T lymphocyte-associated antigen 4
- PMID: 10899917
- PMCID: PMC2193248
- DOI: 10.1084/jem.192.2.303
Immunologic self-tolerance maintained by CD25(+)CD4(+) regulatory T cells constitutively expressing cytotoxic T lymphocyte-associated antigen 4
Abstract
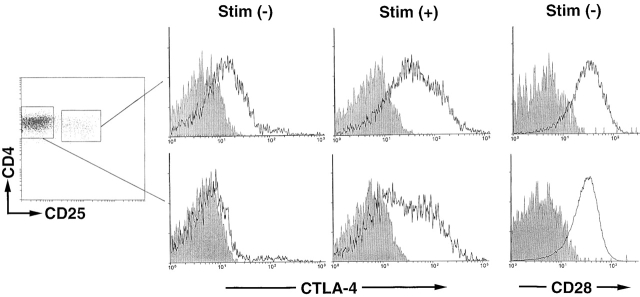
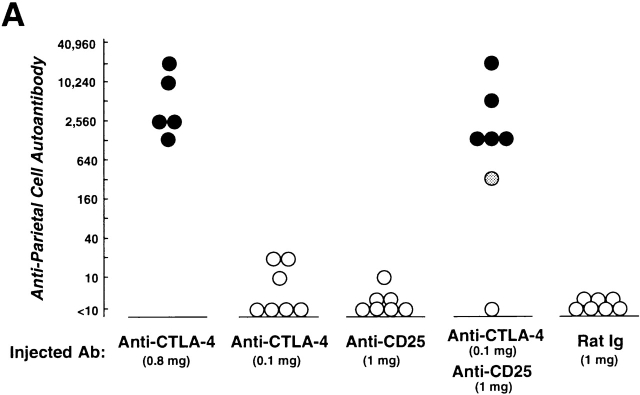
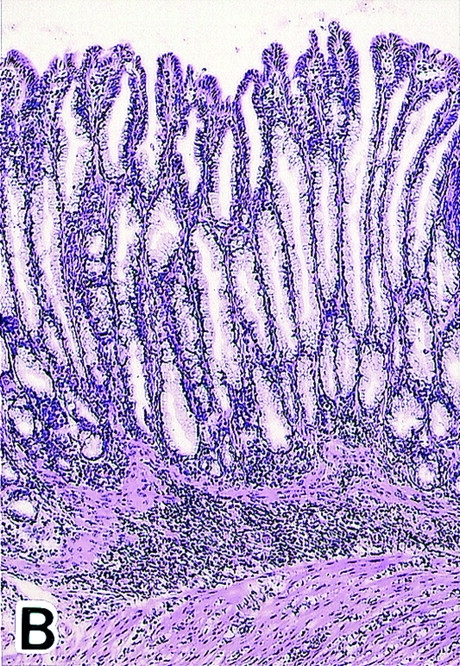
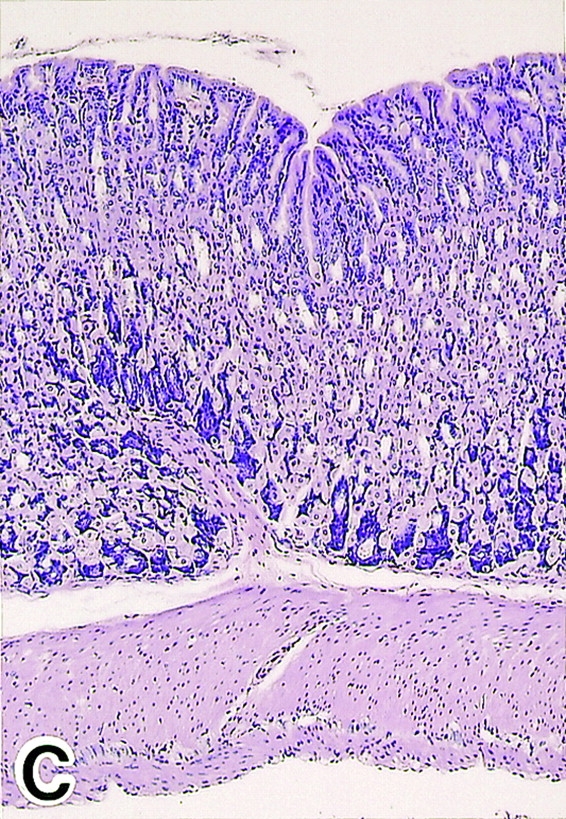
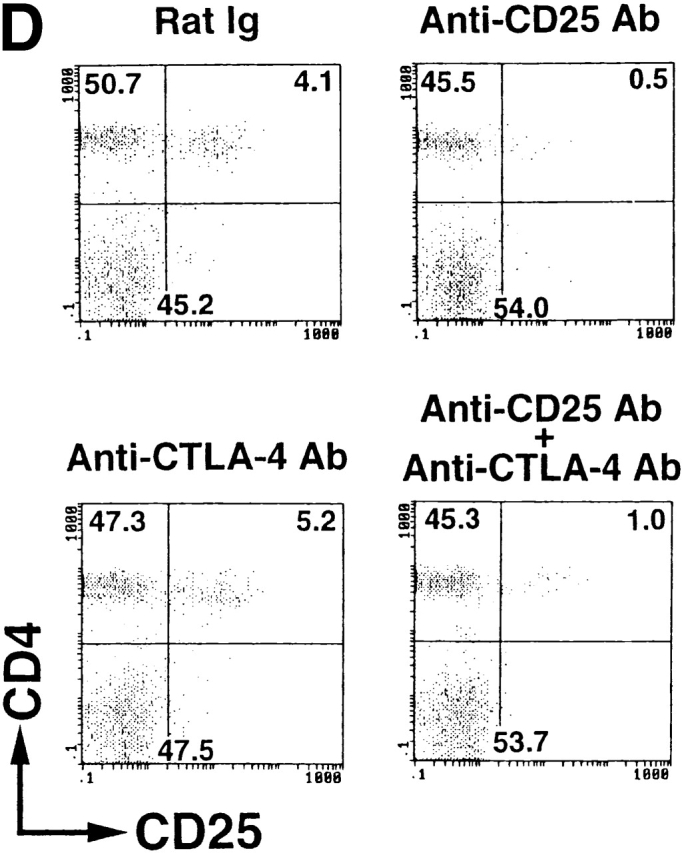
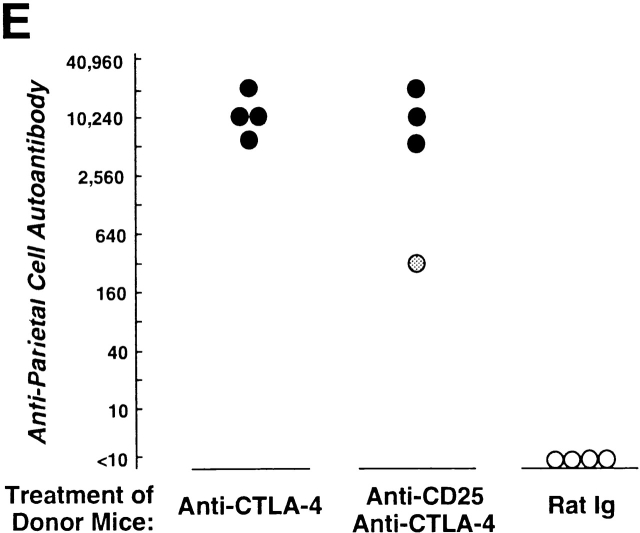
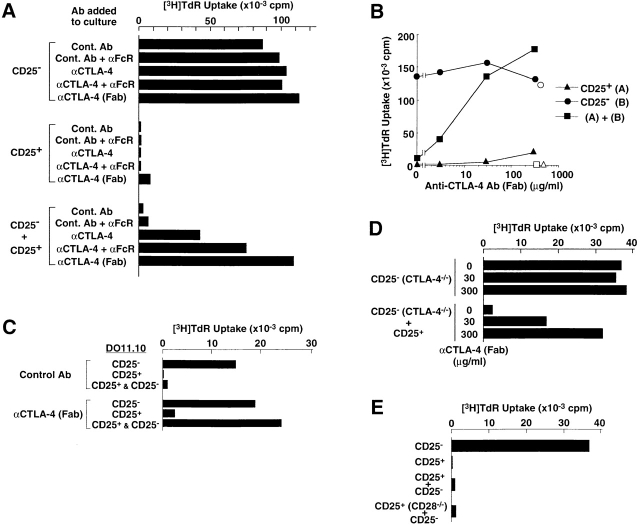
This report shows that cytotoxic T lymphocyte-associated antigen 4 (CTLA-4) plays a key role in T cell-mediated dominant immunologic self-tolerance. In vivo blockade of CTLA-4 for a limited period in normal mice leads to spontaneous development of chronic organ-specific autoimmune diseases, which are immunopathologically similar to human counterparts. In normal naive mice, CTLA-4 is constitutively expressed on CD25(+)CD4(+) T cells, which constitute 5-10% of peripheral CD4(+) T cells. When the CD25(+)CD4(+) T cells are stimulated via the T cell receptor in vitro, they potently suppress antigen-specific and polyclonal activation and proliferation of other T cells, including CTLA-4-deficient T cells, and blockade of CTLA-4 abrogates the suppression. CD28-deficient CD25(+)CD4(+) T cells can also suppress normal T cells, indicating that CD28 is dispensable for activation of the regulatory T cells. Thus, the CD25(+)CD4(+) regulatory T cell population engaged in dominant self-tolerance may require CTLA-4 but not CD28 as a costimulatory molecule for its functional activation. Furthermore, interference with this role of CTLA-4 suffices to elicit autoimmune disease in otherwise normal animals, presumably through affecting CD25(+)CD4(+) T cell-mediated control of self-reactive T cells. This unique function of CTLA-4 could be exploited to potentiate T cell-mediated immunoregulation, and thereby to induce immunologic tolerance or to control autoimmunity.
Figures
References
-
- Thompson C.B., Allison J.P. The emerging role of CTLA-4 as an immune attenuator. Immunity. 1997;7:445–450. - PubMed
-
- Bluestone J.A. Is CTLA-4 a master switch for peripheral T cell tolerance? J. Immunol. 1997;158:1989–1993. - PubMed
-
- Waterhouse P., Penninger J.M., Timms E., Wakeham A., Shahinian A., Lee K.P., Thompson C.B., Griesser H., Mak T.W. Lymphoproliferative disorders with early lethality in mice deficient in Ctla-4. Science. 1995;270:985–988. - PubMed
-
- Tivol E.A., Borriello F., Schweitzer A.N., Lynch W.P., Bluestone J.A., Sharpe A.H. Loss of CTLA-4 leads to massive lymphoproliferation and fatal multiorgan tissue destruction, revealing a critical negative regulatory role of CTLA-4. Immunity. 1995;3:541–547. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
Research Materials
