

Protective effects of ischemic preconditioning for liver resection performed under inflow occlusion in humans
- PMID: 10903590
- PMCID: PMC1421123
- DOI: 10.1097/00000658-200008000-00001
Protective effects of ischemic preconditioning for liver resection performed under inflow occlusion in humans
Abstract
Objective: To determine whether ischemic preconditioning protects the human liver against a subsequent period of ischemia in patients undergoing hemihepatectomy, and to identify possible underlying protective mechanisms of ischemic preconditioning, such as inhibition of hepatocellular apoptosis.
Summary background data: Ischemic preconditioning is a short period of ischemia followed by a brief period of reperfusion before a sustained ischemic insult. Recent studies in rodents suggest that ischemic preconditioning is a simple and powerful protective modality against ischemic injury of the liver. The underlying mechanisms are thought to be related to downregulation of the apoptotic pathway.
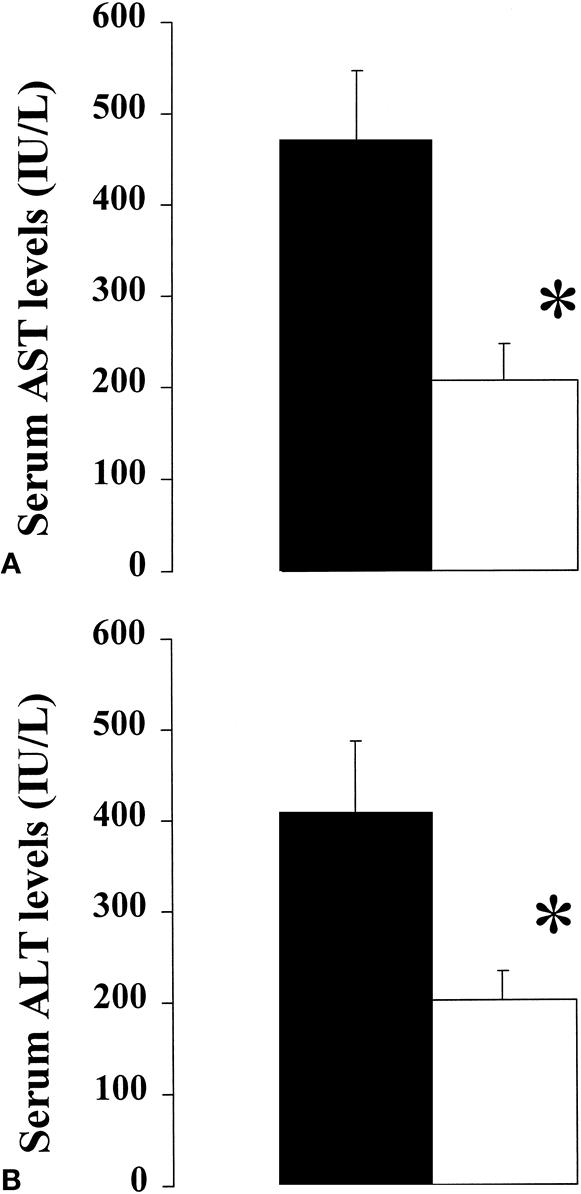
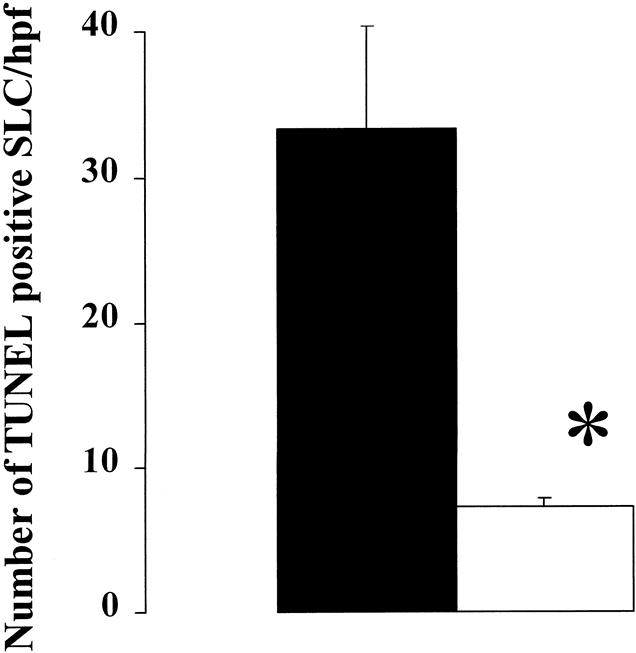
Methods: Twenty-four patients undergoing hemihepatectomy for various reasons alternatively received ischemic preconditioning (10 minutes of ischemia and 10 minutes of reperfusion) before transection of the liver performed under inflow occlusion for exactly 30 minutes. Liver wedge and Tru-cut biopsy samples were obtained at the opening of the abdomen and 30 minutes after the end of the hepatectomy. Serum levels of aspartate transferase, alanine transferase, bilirubin and prothrombin time were determined daily until discharge. Hepatocellular apoptosis was evaluated by in situ terminal deoxynucleotidyl transferase mediated d-UTP nick end-labeling (TUNEL) assay and electron microscopy. Caspase 3 and 8 activities were measured in tissue using specific fluorometric assays.
Results: Serum levels of aspartate transferase and alanine transferase were reduced by more than twofold in patients subjected to ischemic preconditioning versus controls. The analysis of a subgroup of patients with mild to moderate steatosis indicated possible increased protective effects of ischemic preconditioning. In situ TUNEL staining demonstrated a dramatic reduction in the number of apoptotic sinusoidal lining cells in the ischemic preconditioning group. Electron microscopy confirmed features of apoptosis present in control but not in ischemic preconditioning patients. There was no significant difference in caspase 3 and 8 activity when patients with ischemic preconditioning were compared with controls.
Conclusions: Ischemic preconditioning is a simple and effective modality protecting the liver against subsequent prolonged periods of ischemia. This strategy may be a more attractive technique than intermittent inflow occlusion, which is associated with increased blood loss during each period of reperfusion.
Figures


Comment in
-
Preconditioning for protection from ischemic injury: discriminating cause from effect from epiphenomenon.Ann Surg. 2000 Aug;232(2):163-5. doi: 10.1097/00000658-200008000-00002. Ann Surg. 2000. PMID: 10903591 Free PMC article. No abstract available.
References
-
- Wobbes T, Bemelmans BLH, Kuypers JHC, et al. Risk of postoperative septic complications after abdominal surgery treatment in relation to perioperative blood transfusion. Surg Gynecol Obstet 1990; 171: 5962–5965. - PubMed
-
- Makuuchi M, Mori T, Gunven P, et al. Safety of hemihepatic vascular occlusion during resection of the liver. Surg Gynecol Obstet 1989; 130: 824–831. - PubMed
-
- Nagorney DMHJ, Illstrup DM, Adson MA. Primary hepatic malignancy: surgical management and determinants of survival. Surgery 1989; 106: 740–749. - PubMed
-
- Horiuchi T, Muraoka R, Tabo T, et al. Optimal cycles of hepatic ischemia and reperfusion pedicle clamping during liver surgery. Arch Surg 1995; 130: 754–758. - PubMed
-
- Hardy KJ, Tancheroen S, Shulkes A. Comparison of continuous versus intermittent ischemia-reperfusion during liver resection in an experimental model. Br J Surg 1995; 82: 833–-836. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
