

Management of duodenal perforation after endoscopic retrograde cholangiopancreatography and sphincterotomy
- PMID: 10903596
- PMCID: PMC1421129
- DOI: 10.1097/00000658-200008000-00007
Management of duodenal perforation after endoscopic retrograde cholangiopancreatography and sphincterotomy
Abstract
Objective: To evaluate the authors' experience with periduodenal perforations to define a systematic management approach.
Summary background data: Traditionally, traumatic and atraumatic duodenal perforations have been managed surgically; however, in the last decade, management has shifted toward a more selective approach. Some authors advocate routine nonsurgical management, but the reported death rate of medical treatment failures is almost 50%. Others advocate mandatory surgical exploration. Those who favor a selective approach have not elaborated distinct management guidelines.
Methods: A retrospective chart review at the authors' medical center from June 1993 to June 1998 identified 14 instances of periduodenal perforation related to endoscopic retrograde cholangiopancreatography (ERCP), a rate of 1.0%. Charts were reviewed for the following parameters: ERCP findings, clinical presentation of perforation, diagnostic methods, time to diagnosis, radiographic extent and location of duodenal leak, methods of management, surgical procedures, complications, length of stay, and outcome.
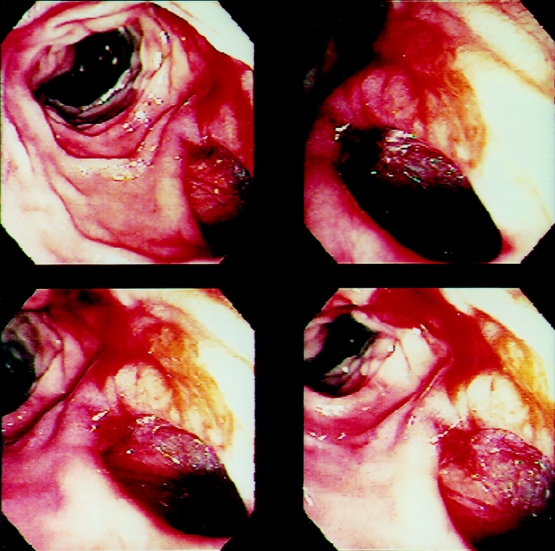
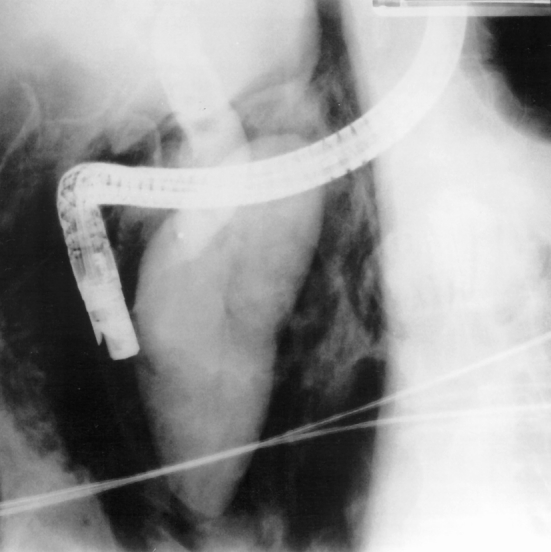
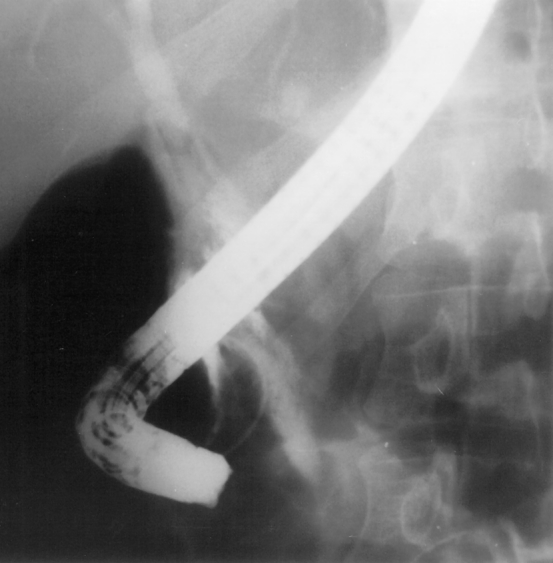
Results: Fourteen patients had a periduodenal perforation. Eight patients were initially managed conservatively. Five of the eight patients recovered without incident. Three patients failed nonsurgical management and required extensive procedures with long hospital stays and one death. Six patients were managed initially by surgery, with one death. Each injury was evaluated for location and radiographic extent of leak and classified into types I through IV.
Conclusions: Clinical and radiographic features of ERCP-related periduodenal perforations can be used to stratify patients into surgical or nonsurgical cohorts. A selective management scheme is proposed based on the features of each type.
Figures


Comment in
-
Re: Stapfer M et al. Management of duodenal perforation after endoscopic retrograde cholangiopancreatography and sphincterotomy. Ann Surg 2000; 232:191-8.Ann Surg. 2001 Jul;234(1):132-3. doi: 10.1097/00000658-200107000-00027. Ann Surg. 2001. PMID: 11420495 Free PMC article. No abstract available.
References
-
- Cotton PB, Lehman G, Vennes J, et al. Endoscopic sphincterotomy complications and their management: an attempt at consensus. Gastrointest Endoscopy 1991; 37: 383–393. - PubMed
-
- Dunham F, Bourgeouis N, Gelin M, et al. Retroperitoneal perforations following endoscopic sphincterotomy: clinical course and management. Endoscopy 1982; 14: 92–96. - PubMed
-
- Elder JB. Surgical treatment of duodenal ulcer. Postgrad Med J 1988; 64 (Suppl 1): 54–59. - PubMed
-
- Cameron J, Kieffer R, Baker R, et al. Selective nonoperative management of contained intrathoracic esophageal disruptions. Ann Thorac Surg 1979; 27: 404–408. - PubMed
-
- Cobb L, Vinnocur C, Wagner C, Weintraub W. Intestinal perforation due to blunt trauma in children in an era of increased nonoperative treatment. J Trauma 1986; 26: 461–463. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
