

Comparison of intravenous/oral ciprofloxacin plus metronidazole versus piperacillin/tazobactam in the treatment of complicated intraabdominal infections
- PMID: 10903605
- PMCID: PMC1421138
- DOI: 10.1097/00000658-200008000-00016
Comparison of intravenous/oral ciprofloxacin plus metronidazole versus piperacillin/tazobactam in the treatment of complicated intraabdominal infections
Abstract
Objective: To compare the safety and efficacy of intravenous (IV) ciprofloxacin plus IV metronidazole (CIP+MET) with that of IV piperacillin/tazobactam (PIP/TAZO) in adults with complicated intraabdominal infections, and to compare the efficacy of sequential IV-to-oral CIP+MET therapy with that of the IV CIP-only regimen.
Summary background data: Treatment of intraabdominal infections remains a challenge, mainly because of their polymicrobial etiology and attendant death and complications. Antimicrobial regimens using sequential IV-to-oral therapy may reduce the length of hospital stay.
Methods: In this multicenter, randomized, double-blind trial involving 459 patients, clinically improved IV-treated patients were switched to oral therapy after 48 hours. Overall clinical response was the primary efficacy measurement.
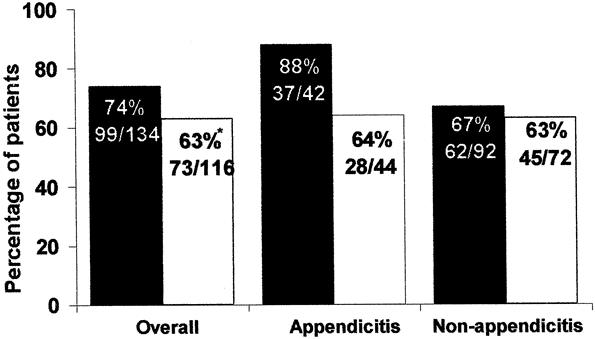
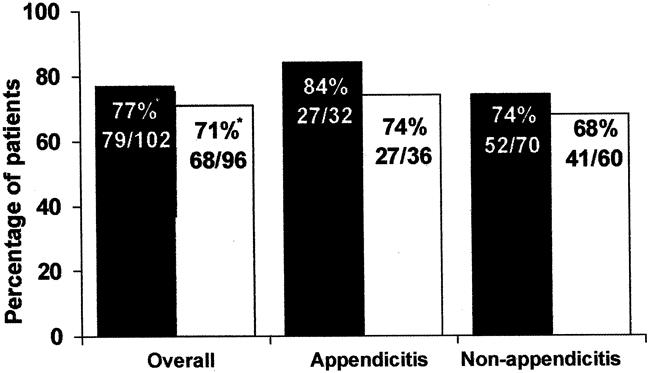
Results: A total of 282 patients (151 CIP+MET, 131 PIP/TAZO) were valid for efficacy. Of these patients, 64% CIP+MET and 57% PIP/TAZO patients were considered candidates for oral therapy. Patients had a mean APACHE II score of 9.6. The most common diagnoses were appendicitis (33%), other intraabdominal infection (29%), and abscess (25%). Overall clinical resolution rates were statistically superior for CIP+MET (74%) compared with PIP/TAZO (63%). Corresponding rates in the subgroup suitable for oral therapy were 85% for CIP+MET and 70% for PIP/TAZO. Postsurgical wound infection rates were significantly lower in CIP+MET (11%) versus PIP/TAZO patients (19%). Mean length of stay was 14 days for CIP+MET and 17 days for PIP/TAZO patients.
Conclusion: CIP+MET, initially administered IV and followed by CIP+MET oral therapy, was clinically more effective than IV PIP/TAZO for the treatment of patients with complicated intraabdominal infections.
Figures
References
-
- Gorbach S, Thadepalli H, Norsen J. Microorganisms in abdominal infections. In: Balowa A, DeHaan R, Dowall V, Guze L, eds. Anaerobic Bacteria: Role in Disease. Springfield, IL: Thomas; 1974: 399–407.
-
- Swenson R, Lorber B, Michaelson T, Spaulding E. The bacteriology of intra-abdominal infections. Arch Surg 1974; 109: 398–399. - PubMed
-
- McClean K, Sheehan G, Harding G. Intra-abdominal infection: a review. Clin Infect Dis 1994; 9: 100–106. - PubMed
-
- Wilson S. Results of a randomized multicenter trial of meropenem versus clindamycin/tobramycin for the treatment of intra-abdominal infections. Clin Infect Dis 1997; 24 (Suppl 2): S197–206. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
